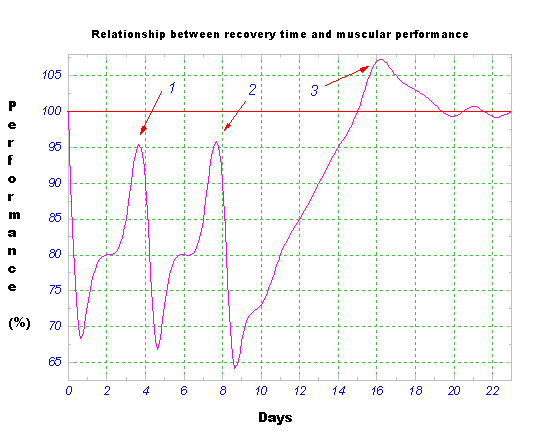
Figure Q.1. Relationship between Recovery Time and Muscular Performance
Questions and Answers about the Power Vision System
excerpt material from the book:
The Secret of Perfect Vision
How You Can Prevent or Reverse Nearsightedness
by David De Angelis
Published by
North Atlantic Books
Copyright © 2008 by David De Angelis. All rights reserved.
I highly recommend that you carefully read this Questions and Answers section. You will gain a much deeper understanding of the Power Vision System techniques and you will find excellent suggestions for how to improve your vision training program and gain faster results. If, after reading this section, you have further questions, please post them on the support forum at www.powervisionforum.com
1. As you state it, this system looks miraculous. Is it science or science fiction?
The Power Vision System (PVS) isn’t science fiction, but science. The system is based upon the training of extrinsic ocular muscles, which are of the striated type, and therefore their physiological structure is equal to that of any other striated muscle in our body (like biceps or triceps). Also the ciliary muscle (smooth type, involuntary) could be efficiently trained with the visual biofeedback technique of the Accommotrac Vision Trainer. This is accomplished by wearing special training lenses and using the well-known concept of blur-driven accommodation. You can find such lenses easily at low cost, and they need be worn only during visual training work.
Ocular muscle training is based on the same principles as any other striated bodily muscle—the system just uses such principles and practices in a different way.
The principles are as follows:
a. The principle of gradual overloading
b. The SAID Principle (Specific Adaptation to the Imposed Demand)
2. Who can guarantee me positive results from training with this method?
This method is simply one of the methods, but it is not a magic pill. If you think you could learn something lying on the divan and watching TV instead of reading an interesting book—or improve your physical condition without “wasting” one single drop of sweat—this book and method will not work for you. The Power Vision System is based on physiological laws and will work well for every single person (who suffers from hyperopic or myopic disorders) and at any age. However, personal commitment is required when using such physiological principles. If you are someone who wants everything (money, wealth, health) without investing time and effort, then this book will not work for you.
If you believe in changes and possibilities in your life, and the power of consciousness offers you the capability to improve and change your situation, then please use the principles of the Power Vision System with trust and perseverance.
3. When I train while reading, I’m not able to make automatic focusing happen, despite the fact that I follow your instructions.
There are two possible reasons:
a. Specifically, in the beginning of training with this method, the eyes are very weak because of low flexibility and strength and coordination of ocular muscles—a situation created while the person wore minus glasses. Over time, the glasses make the eyes “lazy,” “freezing” natural and physiological focusing. The result is “stiff” eyes, which get tired easily. The solution for this problem is to carry out the Power Vision exercises of cyclorotation and fixation at the edges of visual field.
b. The other possible reason for your slow response is in automatic focusing. This could be due to an excessively long focusing distance for that training session. Remember that the load that is imposed on the eyes must lead to an adaptation; it shouldn’t be excessive.
4. When am I supposed to change my training glasses? When am I supposed to train with reading, focusing with higher dioptric power lenses on the training glasses?
The right moment to change the lenses and wear higher dioptric power ones (for example, myopes from +1 to +2, and hyperopes from –1 to –2) is when the text is in focus while holding your reading material with completely extended arms and wearing your old training glasses. The load—the lenses themselves—aren’t a training load anymore because they aren’t strong enough to create the slight “fogging” that is the most important and basic part of stimulating focusing. For hyperopes, when the text is in focus, at too short a distance, use a negative lens or an undercorrection and do defocus training at an higher distance. The solution is to move to a higher dioptric power training lens.
5. I’m not able to go further; my focusing looks as if it were steady at x distance.
Focusing distance must be changed constantly throughout the time of training: the text must be moved to the furthest distance (for myopes) or at the lowest one (for hyperopes) so as to have an efficient stimulus for training by focusing constantly, and then, at that same distance, after opening your eyes widely for about 5 seconds and then blinking, you will notice you are able to focus well.
Focusing improvement doesn’t always go continuously and gradually. You might not have any positive results even after two weeks of training. If you are focusing and carrying out ocular stretching correctly, suddenly you will notice remarkably better and clearer vision.
Keep trusting in the system and keep going with practice (solidifying the little improvements you have already achieved).
6. Can I wear glasses and/or contact lenses and improve my sight at the same time?
Wearing glasses with your current dioptric power prescription (or even worse, wearing contact lenses) could hinder the improvements in training with the Power Vision System. Wearing minus glasses (current dioptric prescription) is the cause of gradual sight deterioration; it is completely opposite to the Power Vision System concept. Training with the Power Vision System relaxes the state of chronic overaccommodation (which is mainly caused by constant near-work compounded by wearing minus glasses). On the contrary, wearing corrective glasses causes a negative state of overaccommodation. Wearing minus lenses should be limited to conditions when they are absolutely needed (when required by the law—like driving vehicles, for instance). If you can’t help wearing minus glasses (above all, in the case of high myopia), then it’s advisable to wear undercorrection.
7. I was told that not wearing glasses or contact (minus) lenses brings about sight deterioration.
False! It’s a mistaken myth that does nothing except make a billion-dollar business—money that goes into the pockets of the optical industry.
It’s completely advisable to reduce a prescription (wherever possible for safety reasons) and limit wearing minus contact lenses and glasses. It’s useful to repeat: Wearing contact lenses and glasses means greater visual stress, specifically in near-work, since this work stimulates visual processes that produce excessive accommodation and converging. This is the main reason that the eye’s focal status moves in a negative direction and becomes nearsighted.
8. I’m afraid of focusing when doing the exercises’ ocular stretching. Could I damage my ocular muscles by forcing them too much?
If you carry out the exercises correctly, with proper understanding of the principle of gradual, symmetric loading and at maximum range, you don’t run any risk. It would be as if we could damage any bodily muscle by training it correctly.
Not only the body but also the mind responds to the change. Fears and doubts have a negative aim. By training ocular muscles, you can improve local blood circulation, which will bring about remarkable functional advantages.
9. I feel some effects while carrying out ocular stretching and also after the training. What should I do?
Whatever the muscular training, if it is carried out with untrained musculature, it can cause some discomfort. It means that you are overloading your eyes. Such gradual overloading will increase your eyes’ performance, improving your sight and decreasing myopia.
10. I don’t have time to do the exercises.
You can train your eyes at any moment throughout the day, and just a few rotations and symmetric movements are enough. You don’t need to get your car and go to the gym, and neither do you have to shower after training.
11. Where can I buy training glasses?
At an optician’s or at any other shop that is supplied with them. Don’t waste your time explaining why you need them, because you could be laughed at or even persuaded that such glasses are “just an illusion.” Demand your sight!
12. Who is guaranteeing the final result of restoring clear, distant sight?
Nothing is sure or guaranteed in our life. Nobody can guarantee your success. The only thing you can do is to trust in the method and persevere in doing the exercises, day after day.
13. Does this method work well only for myopia or also for other visual disorders?
My personal experience is with treating and healing myopia—but it doesn’t mean that other visual disorders can’t be treated with this restorative method.
The exercises of ocular stretching are surely useful and beneficial for training for focusing at a distance, but the very same principles can be used successfully even in the opposite way, for focusing at a near distance (as it happens with sight worsening). The only difference is this: we can use the same principles to improve our sight (gradual overload of focusing, either by moving the focusing point away for myopes or bringing it nearer for hyperopes) that are opposite to the reasons for sight deteriorating (both myopia and hyperopia—like constantly wearing glasses or contact lenses; too much near-work).
Obviously, everyone should carefully evaluate his or her own sight and its conditions and carry out the training program that is the most suitable. This is like a schedule for athletic training that must include the athlete’s needs concerning his or her own bodily characteristics. The principles are the same, but they must be adjusted to one’s personal needs. However, I’m sure that even astigmatism could improve from ocular muscle training, since such training brings about a restoration of the balance between agonist and antagonistic ocular muscles.
14. Does this method have anything to do with the Bates one?
Dr. William Bates is surely a most important person for having turned our attention to the fact that the process of accommodation is closely linked with ocular muscles’ perfect functioning, and that the shape of the eyeball can be modified by contracting and relaxing the extrinsic ocular muscles and changing focal point on the retina. (This is your refractive status, which is measured by using a trial lens kit (phoropter) by you or your optometrist.)
Our method is different than the Bates Method, because in the Power Vision System the muscles are trained by using the two main features that rule muscular performance (here, focusing). These two factors are strength and flexibility. Bates insisted on a “light” approach of relaxing exercises (or movement). The Power Vision System insists on complete improvement of the most important characteristics and properties of ocular muscles: strength and flexibility.
To clarify, it’s like the difference between (light) yoga and artistic gymnastics. The analogy is the situation where the athletes are trained well and their muscles are very flexible and strong. This is not by accident. The gymnasts are endowed with what’s called “refined dexterity” in movements, which requires extremely precise coordination and motor qualities. Ocular muscles need this extraordinary quality—refined dexterity—to fulfill as complex a task as focusing is.
This phenomenon is underestimated, since we were born with this natural motor ability (in our eyes as well), but long, hard work is needed to become a gymnast. When you have a visual error, and you eventually reach 20/20 vision, your success is as though you obtained a 10/10 score at springboard. Surely, it’s not an easy task. Undoubtedly the path to reach 20/20 exists, and the furrow has already been plowed, in my judgment.
15. I have high myopia. As far as restoring my sight gradually and naturally, what are my chances of improving my situation since my present clinical state is the following: For eleven years my diopter has always been the same:
Right Eye: 11.0 diopters Astigmatism 1.5 at 180 degrees
Left Eye: 6.0 diopters Astigmatism 1.0 at 180 degrees
Since last year, it has been:
Right Eye: 13.0 diopters Astigmatism 1.0 at 125 degrees
Left Eye: 6.75 diopters Astigmatism 1.75 at 165 degrees
But I still don’t have a new pair of glasses.
As long as the technique is used correctly, this system works well. The limit is imposed by the person who trains with the system. When you notice the first visible (literally) improvements, you will easily understand that it’s just a matter of practice. It is true: the system requires great trust (in order to break one’s own skepticism and achieve the first positive results). Just imagine yourself taking a degree in engineering (the commitment and effort required), but in this case your own eyes and your sight are on the scales.
I’ll give you an example related to mechanical-architectural engineering to help you understand it more clearly. Understand the concept of gradually building (brick by brick) the difference between a middle-sized building and a castle. The first step depends on the worker’s engagement (in our case, it depends on your commitment to doing the exercises, which are similar to the bricks) and on the time you spend in doing the exercises. Surely Rome wasn’t built in a day, but I think, when dealing with a very important thing (like your vision), you must be very responsible and do it with great commitment.
In my example, I would be both the engineer and architect. The Power Vision System has established the ways of construction and I’ve checked them out by myself. Do something for your eyes while you still have the time.
16. I’m hyperope (+ 4 right eye, and + 4.50 left eye) and astigmatic. I kindly ask you to explain to me what your method would consist of in my case?
Hyperopes have problems in focusing on near objects, since hyperopia is the opposite of myopia. The Power Vision System is based on fundamental physiological principles, which are common to both refractive errors. (A positive refractive status is hyperopia and a negative refractive status is myopia.) The most important and basic principle for the Power Vision System is the SAID Principle (Specific Adaptation to the Imposed Demand). This principle is well known in physiology (and in sports training); it means that the body has a natural ability to get used to induced stimuli.
Let’s take an example from sports: an athlete who trains his or her muscles and physiological systems (for example, cardiovascular and respiratory systems) with induced loads in specific training. Such loads will cause a bodily response—an adaptation. In bodybuilding, for example, such a response is represented by anabolism, actually, by muscular hypertrophy. In the case of treating refractive errors like myopia and hyperopia, the stimulus (the key factor for creating bodily adaptation, in this case of the eyes) must be specific and suitable for achieving the desired results. It’s interesting to point out that such a stimulus must be masterly directed (so as to have positive results—recovery— and in our case, it means visual error regression until, in due course, a complete recovery). Otherwise, in the opposite case, it could cause the opposite results.
Now, you can see that every stimulus, badly imposed (directed) to the visual system, like wearing lenses or glasses in conditions when the eye could view correctly without them (for example, a hyperope who views distant objects wearing positive “correcting” lenses, ruins his own sight, causing overcorrection, which has negative effects on his proximal accommodation when he takes off his lenses). A completely opposite process works in case of myopia: a myope who wears glasses or contact lenses in near activities, worsens his refractive state furthermore, creating overaccommodation. When he takes off his glasses, his distance vision will be even worse.
The SAID Principle must have specific and differentiated use for each visual error, although it works well for both errors—myopia and hyperopia.
There’s also a solution for your light exo/esophoria: to restore perfect ocular muscle symmetry through specific training of your extrinsic ocular muscles. Do you know that these little muscles are of the striated type and have the same structure as your biceps muscle (sarcomere: actine, myosine)? When you understand it, you’ll be able to figure out that they have the same characteristics in training as any other bodily muscle. The laws are equal, but their use in practice is specific and different. The treatments should be directed, at first, to using Natura Medicatrix and natural laws before using any artificial means.
17. I’ve already achieved improvements and stability in my vision. Will I be addicted to another therapeutic treatment? How do you check for muscular asymmetry? I completely understand the concept of doing the exercises and trust in the technique. Is it a matter of lifetime engagement (doing exercises for better accommodation) or is your technique the “resolute” one, through which, after a certain, necessary period of doing the exercises, a myope can restore his visual qualities, partially or completely, but permanently?
The system gives permanent results, unless (so be careful) you subject your visual organs to those negative stimuli again (the stimuli that are ill omened for ocular accommodative capability).
Let me give you one simple and clear example: the myopes suffer from chronic overaccommodation, due to near-work (functioning makes the organ and body get used to the imposed stimuli, both positive and negative [the SAID Principle]). According to these laws, you have been worsening your sight for years, wearing higher and higher negative dioptric power lenses. When you lessen this state of overaccommodation (until reaching the normal, clear, distinct sight—the emmetropic state), you must only follow and respect simple behavioral rules of “visual hygiene.” Obviously, if you put your minus glasses on again (with your ordinary dioptric power lenses), after having worked with the Power Vision System to relax the state of chronic overaccommodation, and then spend a long time in near-work activities, all the necessary conditions for creating myopia will be created again. The target is to give up certain negative habits and restore the balance of the extrinsic ocular muscles. Without explaining the theoretical part completely, try this simple test that could help you become aware of your ocular muscles’ asymmetry (imbalance between strength and flexibility, and consequently, coordination).
1. Stand in front of a mirror, and without wearing your glasses fix on the top of your nose. You must be as distant from mirror as permits you to see your nose well.
2. While maintaining binocular fixation, carry out symmetric movements of your face (for example, lower your chin, turn your head toward the right as much as you can, then toward the left as much as you can). Such movements (we can compare them to cardinal points) must be united into one single movement of head rotation, keeping fixed on your nose). The movements you carry out must be symmetric and without twisting. At a certain point, you’ll eventually see the fixed image double (the top of your nose). This means that your ocular muscles are asymmetric, and this condition reflects on convergence (the prevailing factor in myopia) as well as on the capability of focusing at Central Fovea (the most sensitive retinal part). The result: blurred vision due to the lack of the ocular muscles’ coordination (are you able to keep fixing on a very fast object?) and due to the saccadic eye movement slowing down.
Your eyes should undergo specific rehabilitation with the specific exercises. The exercises proposed in this book are founded on physiological laws and you can find the sources in any scientific bibliography.
18. From what I understand, your “method” is based on intelligent use of positive lenses for myopes and/or undercorrections. The lenses should have a different dioptric power in order to follow sight evolving, and the only problem I have at the movement is getting them. Am I supposed to buy an ophthalmologic kit, or is it better to have a new pair of glasses made from time by time?
No ophthalmologic kit. You can easily find the glasses you need at a pharmacy or drug store but also at large stores like K-Mart or Wal-Mart (at $10 to $15). You’ll need glasses +1, +2, and +3 (if you’re myopic). The combination of these lenses (for example, +3 with +2) will lead you forward in your training by increasing the stimulus. Later on, when you reach a higher level, you can add +4 lenses, creating +7 stimulus together with +3 lenses. You can buy such glasses at a low price—much lower than for a pair of ordinary minus-prescription glasses, which cost $100 or higher. Training with such glasses will lead you to throw away your glasses forever (no matter what kind you are wearing at the moment) and, even in the worst case, to improving your sight a great deal. It depends on your practicing with commitment. The method and means (actually the technique) does exist!
19. I’m a bit of a skeptic. I’ve been doing the exercises. I was taught by a therapist. I started 15 months ago (I wore contact lenses–4.75 and –4.50) and now I wear –2.25 and –2.00 ones. My recovery has been going very slowly, but it does goes on. Now I’m doing it by myself, repeating a few exercises that my teacher has taught me. I think it’s not the Bates Method, because I’ve read many books on the issue and I know that the Bates Method is based on relaxation. I desperately want to see well without the help of any means. I’ve spent a lot of money on glasses, contact lenses, liquids, therapeutic sessions.
I’ve always been interested in learning—above all else—what I need. I would also like to speed up my sight improvement (if possible). I’m very interested in all that you say, but I am a skeptic about buying something without having examples of its effectiveness. Please give me some examples of your method so I can decide whether to buy it or not.
Being interested in learning and knowing more has caused me to purchase many a rip-off. Once I bought a book on “visual reeducation” for $25. Twenty-five dollars for twelve pages! Using the same metric, the Power Vision System should be offered at a substantially higher price.
I think you are going in the right direction, since you’ve improved your sight so remarkably. I think your trainer is excellent.
As I’ve written, my system is based on:
a. Using the lenses of opposite dioptric power to the ordinarily worn ones (for example, myopes should wear positive instead of negative lenses). Such a system acts on the ciliary muscle’s over-accommodative state. Keep in mind: There’s a specific way to graft focusing (normally it is an automatic process. The system is called ocular CRB movement).
b. Increasing coordination and ocular mobility. Do this simple test: Fix your vision at the top of your nose, standing in front of a mirror at 3 feet distance (if you are able to see your nose well from that distance, otherwise come nearer to the mirror). Carry out symmetric rotations at the maximum range of ocular movement, turning your face (for example, as far up as you can,toward the left, toward the right, always as much as you can)while fixing on your nose.
You will see that in some parts of your visual field (if the movements are symmetric and at maximum range), the image will become double (or, at least, you’ll have trouble maintaining a fusion of the fixed point, in this case of your nose). It means that point b, through the exercise of muscular working at maximum range, will lead you to remarkably better fusion,which is needed—and is basic for perfect focusing, since the image must fall on the central fovea (the most sensitive retinal part);otherwise it would be blurred (it depends on how far from the central fovea the image falls).
Keep going on this way, and trust in what you’re doing. When you see well again, not only will you see clearly, but you’ll also be aware of having done something really special in your life and you’ll understand that everything is possible if you believe you can get it.
20. I tried the Accommotrac, getting some good results, but not as good as I expected. I’m a myope at –0.75 D in my right eye and–1.25 D in my left eye. Why should your method work better than the Accommotrac? I’ve also read Bates. I never wear glasses, and my sight hasn’t worsened a lot in these years, despite the fact that I’ve been working at computer a lot.
I’ll do my best to explain to you about Accommotrac Vision Trainer limits—and why PVS works well. The eyes must point at central parts of the visual field in training with Accommotrac: your gaze must be directed and “blocked” toward ahead. This very thing happens while wearing glasses, but then, the eyes are not “stimulated” to view at the limits of ocular movement range, which is much wider than the ordinary one used when wearing glasses. This kind of functioning is abnormal,and, with time, it jeopardizes the extrinsic ocular muscles’ functioning.
Your ocular capability is characterized by involuntary ocular movements that are extremely fast—so called saccadic movements. When basic ocular endowments become weak because of working at a limited range (as it happens wearing glasses or in training with Accommotrac), the eyes gradually lose their full saccadic movements’ functioning and, consequently, their focusing ability.
The Accommotrac works well, but it has its own limits, which could be overcome by supplementing it with the techniques as described in PVS.
I think it’s important to point out that training by use of a focusing machine could be replaced with a system that isn’t based on sound but on proper visual biofeedback. The latter system consists of a clever use of the lenses that are opposite to the visual error (if you’re a myope you should train wearing the lenses for hyperopes or train with undercorrected glasses). However, nothing could be improved by the simple wearing of the opposite lenses because there is a very precise technique to be followed.
The most important thing is personal commitment and effort in carrying out the Power Vision System technique for some time. We should remember the principle: Knowledge is worthless unless you use it.
21. What is your advice for using training lenses? What dioptric power should I start with? I have myopia and strabismus. My right eye is –6 ast. and my left one is –6.25 ast. –2.25.
a. Where could I buy training lenses? Are they the kind I can find for $15 to $30 in the stores?
b. What dioptric power I should start with?
c. Are the training lenses to be used in addition to my present correction
or apart?
d. Am I supposed to feel some muscular “stiffness” in order to see that the CRB movement exercise is carried out correctly?
You are quite lucky since your myopia is almost equal in both your eyes.
a. You can find the glasses you need at an optician’s, drug store,or in most large stores.
b. and c. As for dioptric power, you should be able to train withreading a book or newspaper, creating a state of slight fogging.
Try to create it without lenses, while reading. Try to move thebook away from your eyes until you create this slight fogging. Then, carry out the CRB movements, and, in the end, blink, to relax your eyes.
Important: You must create a certain, basic ocular strength and flexibility through stretching at maximum ocular range. At the beginning, your self-focusing system (now “frozen” because of wearing glasses and contact lenses for years) will be reluctant to work, but trust and believe in the system and keep going on.
At a certain point you will see that after CRB movements all that was previously blurred now becomes clear. When you understand this principle, everything will be only a matter of great patience and perseverance.
The eyes get used to the lenses with time, and therefore you must increase the stimulus (either moving the text away or increasing dioptric power of your training lenses).
d. The feeling of this “work” is very personal. However, by opening your eyes wide, you will feel some eye stiffness.
You must try several times, changing your lenses until you find the most suitable ones. Start without lenses (if you can) or wear your present glasses with another additional pair over, with positive lenses +1 and +2. You must create fogging before carrying out CRB movements.
22. I’m thirty now and probably the “shape” of my eye (if hyperopia depends on the shorter eye) can’t be modified a lot, at least, not as much as in childhood: is this true or false? Despite the present boom of refractive surgery and the associated billion-dollar business, I’m suspicious about such methods. I’m a hyperope with +4.5 for my left eye and 20/20 in my right eye. Lately I’ve been thinking of starting to wear a blindfold over my right eye to force the left one; as once, a long time ago, I was ordered to do so by an oculist—but probably the “shape” of my eye can’t be modified as much as it could be in childhood.
Is it possible by practicing with your method that we can get positive results? Is there any limit for practicing your method at an “elderly” age?
Just one question more—but I wouldn’t like you to misunderstand it: Why do you want to sell me your book, if you are pushed by so great a praiseworthy and altruistic desire to spread and share your discovery and your knowledge?
I can understand your doubts completely. You say, “I’m thirty now and probably the ‘shape’ of my eye can’t be modified as much as in childhood. . . . ”I ask, Who has said that? What kind of science is that statement based on? Who has ever stated that muscular tissue can’t be modified or get used to suitable stimulus through specific exercises? People who deal with such issues professionally have no time to explain to you certain things (if they even know about them). Sometimes it’s easier to put a pair of glasses onto someone’s nose than to spend time explaining and above all teaching you about this method. Usually, the person who checks your sight also sells glasses, and not everybody is ready to work their way out of their visual defect: they prefer to accept the opinion that nothing can be done to resolve refractive errors. Everybody is free to choose what he wants and likes, even though it may only be a temporary“ quick fix.”
Age doesn’t make any difference for getting positive results in working with the system: PVS is based on physiological concepts that work well at any age. As long as you are able to “command” and control your ocular movement, you’ll also be able to restore your ocular symmetry and consequently your “central fixation”—which is fundamental for clear, distinct vision.
23. I have some questions on the exercises:
a. Does your method work well for strabismus (esotropia orexotropia)?
b. Should the rotations in stretching be slow or fast? For how long a time am I supposed to hold onto a certain position in stretching without rotations?
c. In the advanced training program, does “twice” (in the exercises)mean that I must put my eyes in a certain position two times?d. Dioptric power between my left and right eye is 1.5 grades (0.50 and 2.00). I’ve found out that my better eye views for the “bad” one and that the latter is getting lazy. Since I think it’s hard to bring both eyes to the same visual acuity, do I run any risk of having one of my eyes idle, which would become lazy with time and consequently would bring about ocular defect worsening? As for training for focusing—could it be carried out with only one eye(the lazy one), covering the other?
e. I read about a guy whose myopia was very high, but he decided not to wear lenses and his sight improved (despite your statement there’s no adapting without fogging). What do you think about this story? If I gave up everything, became a farmer, and did no exercises, wouldn’t my sight improve? Then if I went on a mountain to view the landscape, wouldn’t my ocular acuity improve?
The system works well for focusing and, above all, it works completely. The exercises provide high ocular coordination and a gradual restoration of focusing.
I’ve tested the system by myself and I’ve had great results—I’ve defeated my myopia. Therefore the system surely works well also for hyperopes, considering that the means of intervening are the same: increasing the ocular ability of placing the image on the most sensitive retinal part—the central fovea—together with the clever use of training lenses.
a. As for your strabismus, I can’t guarantee its complete healing since I don’t have complete evidence or proof. It does not mean that the system couldn’t work for decreasing the strabismus gradually: including better oculomotor muscle functioning(extrinsic ocular muscles) together with resultant better focusing that are likely to bring about astigmatism decreasing, at least indirectly. But I can’t guarantee it. It’s up to you—the reader—to prove and confirm such a hypothesis, trusting and practicing in the method.
b. The speed in doing the exercises of ocular stretching should be slow and controlled. Such kind of stretching is called “active static stretching.” Ocular muscles’ lengthening and stretching happens, in a certain portion of visual range, by means of agonist (contracting) muscle and its antagonistic (lengthening/extending) muscle. Every muscle could be both agonist and antagonist, depending on a movement it’s carrying out at that very moment.
When you look down, some of your ocular muscles are agonist,and the others, which are placed in the opposite ocular section,are antagonist. In the opposite case, when you look down,the exact opposite thing will occur. This “stretching out” is caused by shortening and contracting the opposite muscle(strengthening); therefore the muscles are to be contracted with a certain intensity.
Use rotations and slow, controlled “pointing,” focusing on those parts of visual field where it’s harder to carry them out and where we feel a “block” or a trough movement (such phenomenon proves the importance and the need for restoring exact local muscular symmetry to bring about more precise pointing and focusing).
c. I meant full rotations—the entire turn each one: two rotations with your eyes opened and two with closed eyes. The purpose is a kind of “warming up” for your ocular muscles so as to make them ready for further exercises. Training protocols depict the standard way. You are allowed to adjust them to your own needs. For example, if in one part of your ocular range you notice double vision, which reveals muscular asymmetry, you must stay in that very portion of visual range. The training routine in PVS is aimed at creating possible ways of working with higher and higher intensity. A period of time is needed for whatever kind of training you carry out, so that you can do it easily—even at the advanced level.
d. Your fear is reasonable. The difference in focusing ability between your two eyes tends to prevail for the “better” eye’s vision. The final result is that your brain tends to use the perception of the more healthy eye, gradually making lazy and worsening the less capable one.
A solution exists: to first train the eye that suffers from a greater visual defect—by blindfolding your “better” eye. Your ability in focusing will gradually improve with this procedure—and little by little, each will become equal to the other eye’s focus. Only at that point can you train both your eyes together at the same time.
Such a procedure is aimed at avoiding suppression of the“ worse” eye and consequently the possibility of its becoming lazy. However, you’ll have great advantages and positive results from this work.
e. Many famous and important authors (like Aldous Huxley and William Bates) have proved to themselves and their patients a better focusing ability.
All that has been proved about sight clearing after giving up the wearing of corrective lenses can’t focus and living “in the open air” isn’t a secret, and it is proven in many studies on near-point stress (due to overaccommodation) and behavioral reasons for myopia. The seminal study carried out with Eskimo families was by Francis A. Young (1969), titled “The Transmission of Refractive Errors within Eskimos Families.” The fogging during the exercises of focusing with the lenses on must be light, otherwise our brain would consider focusing an impossible duty and consequently wouldn’t even try to do it. I’m referring to the phenomenon of blur-driven accommodation. It’s true that when you are outdoors and have less near-point stress (overaccommodation), your sight (refractive status) will get better. This has nothing to do with the importance of the training stimulus that must be imposed on the visual system and it is needed to achieve focusing system adaptation. Both living in the open air and slight fogging are needed to induce a “positive” adaptation of focusing system and resultant distance vision clearing.
24. When I’m able to focus a text well, holding it with completely extended arms, does this mean that I’m supposed to change my plus lenses? For how long a time should each stretching position be maintained while carrying out the exercise of stretching (in seconds)?
a. Starting from focusing: I put my glasses on (I always wear undercorrection, when studying or working) and then I put a +1 additional lens over my correcting lenses, move the book as far away in order for the letters to be slightly blurred, carry out CRB movements, stretching out my eyes and eyebrows as much as I can and have the letters come into focus—even if not perfectly. Am I right? Then, I take off the +1 additional lens while blinking, wait for some seconds, put the +1 additional lens back, move the text away until the letters are slightly blurred, carry out the CRB movements and so on. Am I carrying it out correctly?
b. Am I supposed to keep my gaze fixed on certain details or I can space it over the page?
c. Should I change the plus additional lenses once I’m able to focus the text well, holding it in completely extended hands?
d. Passing to static gymnastic: I take off my glasses, because I can’t focus anything well if I wear my glasses, and carry out the exercises at extreme positions of the visual field; one of my eyes views through the lens, but the other doesn’t.
e. When fixing on a point and turning my head till maximum ocular tension (for example, toward the left, as much as possible), at a certain point my right eye vision is completely, or partially, covered with my nose: is it okay, or too much?
f. For how long am I supposed to keep in one stretching position(as well as all the positions in the exercises of stretching), in seconds?
I’m pleased and willing to answer all your questions:
a. The sequence you are carrying out is correct and there’s no need to take off the additional lenses (+1 in your case, but dioptric power of the additional lenses would be +2, +3, +4, at a higher stage in practicing this technique, or if you were treating hyperopia, the lenses would be negative). On the other hand, if your myopia were low, you could train with training lenses even without putting them over your ordinary, correcting glasses, wearing only training lenses. The explanation for the latter is that your myopia is low (about 2 diopters per eye), the fogging(driven for reading the text) is “reasonable,” even without your present dioptric power glasses.
As reasonable, I mean the method or technique that lets you create slight fogging and focus on the text without holding it 3–4 inches from your nose (as you should do if your myopia were high and if you immediately trained without your ordinary lenses but with the opposite sign). As for high myopia, it is necessary to put the training lenses over the ordinary ones; then, as your focusing is improving, you take off your ordinary lenses and/or even increase the dioptric power of your training lenses. The adaptation is inevitable, otherwise we wouldn’t be able to explain gradual sight worsening.
You don’t need to take off your training glasses after CRB movements.
b. The gaze can move all over the paper, but if you want to read the text you are training with, you must “point” the line and the letters you would like to focus on, as when reading normally.
c. Yes, but it’s a matter of convenience. When you reach the stage of training with reading, wearing additional +1 lenses, and holding the text in completely extended arms, you must change the lenses and use higher dioptric power training ones, simply because, otherwise, it would be hard to read the text at a further distance.
The simplest thing to do is to increase the training load for your eyes, putting higher dioptric power training lenses over the others. Now you can see that the length of your completely extended arms that you take as a limit for the present training lenses is a matter of convenience and, therefore, the sign to change them.
Keep in mind: In the case of hyperopia, the text should be brought nearer gradually—and the training lenses could be changed for higher dioptric power ones (passing from –1 to –2 and then to –3, concerning your refractive error). When you bring the text too close to your nose, there’s no slight blur:
then, since the load doesn’t exist anymore (because your eye has gotten used to training lenses, improving its focusing ability), it will be necessary to rebuild the load with higher dioptric power lenses (the training ones).
d. Yes, you must take off your glasses when carrying out the exercises of ocular stretching; otherwise these glasses would hinder your peripheral fusion and pointing. At this early stage, you must maintain ocular fusion (opposite to splitting). This is the aim of these exercises—to restore the symmetry (flexibility/strength ratio) of extrinsic ocular muscles. In short, maintain the fusion of the fixed point at the edges of the visual field.
e. Your nose shouldn’t jeopardize your training, and you must stop your glance before one of your eyes becomes covered with your nose; otherwise you can’t tell whether your eyes are in the state of fusion or splitting.
f. I need to explain some concepts on contraction intensity and muscular work. As for muscular work, the intensity is the relationship between quantity of load that is moved in a time unit. In the case of isometric contractions (when the muscle is contracting against a steady resistance), and in our case, it is impossible to give you precise suggestions on the factor of contraction intensity.
How can we avoid this merely theoretical factor? How can we be sure that our eyes are always subjected to the load that is suitable to create muscular adaptation? The answer is in perceiving the level of muscular work you are carrying out. Muscular work (the intensity of contraction) depends on your willingness: you must fix at the extreme point of your visual field as if you wanted to overcome that very range of movement.
The time? 10 seconds or 1 minute—it depends on how much muscular work you would like to carry out. The greater the intensity, the more you bring about muscular recovery—strength increase and better ocular muscles’ functioning. Don’t worry if you didn’t understand some of these technical explanations. You aren’t supposed to understand cardiovascular circulation functioning in order to make your heart work. All that you are supposed to do is to use and practice the technique.
25. How about it: you state that we shouldn’t wear special lenses more than 2 hours per day (in the intense program)! Why?
The answer to your question is in the capability of our body to get used to different, induced stimuli: Exposing any physiological system to specifically and systematically repeated stimuli inevitably leads to changes in the that organ’s functioning. Regarding focusing, it means that specific exercises lead to modifications and consequent positive changes in focusing. So as to trigger the body’s capability of getting used to the induced stimuli, we need a stimulus of certain intensity, which could be empirically quantified as training time. Following the technique correctly, the most important factor is to calibrate the stimulus intensity so as to ensure it will be enough to trigger the adaptation without being excessive and therefore “unproductive.” It’s completely useless to overcome the adaptation threshold of any physiological system; therefore, it would be useless if someone trained with training lenses or did the exercises of ocular stretching for 24 hours. You can’t achieve improvements, since the body (and mind) have to take their own time for this adjustment or change to take place.
Imagine an athlete who is lifting weights and wants to increase his strength and muscular mass. He would practice according to his own training program for strength increase, lifting heavier and heavier weights (intensity—otherwise, after a while, it wouldn’t be a training stimulus at all). If he trained for 3 hours a day or 8 hours a day, his performance wouldn’t increase; excessive stimulus could even be self-defeating, jeopardizing recovery and body adjustment.
I’ve set up a 2-hours-daily training limit for the advanced program, since it’s estimated as a maximum stimulus to achieve the improvements fast and without jeopardizing your focusing ability.
The eyes need a maximum stimulus that is both suitable for training and also creates positive adaptation, like a positive focus change. The body needs time to get used to the exercises, as does your mind, which needs time to get used to perceiving the world that now appears clearer and with enhanced shadings. The visual process isn’t merely a physiological one, but one that involves deeper parts of the human psyche and our relationship with ourselves and with others. The way we relate to ourselves is with respect to our mind. Am I not said to be myopic-minded? The body is the soul’s mirror: when you understand it you will also understand how to work on your body. Your mental and emotional horizons are widening toward spiritual and holistic healing—and this involves all the states of “being” and not only the physical ones.
26. How long will it take to recover from my 4.5 D in my left eye? How long did it take you to recover?
Nobody can tell you in exact terms the time needed to restore your focusing ability; it’s also very hard to estimate it, since it depends on many factors—your initial refractive state, the kind of work you are doing, your visual environment, and the kind of effort you are willing to make. Also included is time you spend using your “protective” lenses and your personal verification of results by checking your own eye chart.
I can say that the time you need to improve your sight depends on the quantity of your training and, above all else, on wearing your “preventive” glasses.
Let me explain further: if someone trains 5 minutes a day and someone else trains for 20 minutes, obviously the time they need to reach the flashes of distinct, clear vision is different. It’s useless to do the exercises and then spend all the day at a computer, wearing your minus glasses, because in such a case overaccommodative stress (proximal stress produced by the minus lens) persists. One thing is certain: the time needed to get improvements is much shorter than the time it took to worsen your sight (which induced your present dioptric prescription).
Being supervised by an optometrist or an ophthalmologist, you can start to do cyclorotation: slow and concentrated on the present maximum range of your eyes, and symmetric. Later on, you can start doing the exercises on retinal defocus so as to bring about a better refractive state. As for this, you should take advice from your physician.
27. Why does it take less time to achieve better visual acuity with the Power Vision System than to notice sight worsening, that is, wearing minus lenses for myopes?
You can expect faster improvement in such cases if the program of sight rehabilitation is carried out correctly: at first acting over muscular properties and the symmetry of oculomotor muscles, and later on over suitable retinal defocus, constantly following the rules of visual hygiene. In such case, the improvements are faster than when wearing minus lenses for myopes, because of wrong use of hyperopic retinal defocus.
When we are subjected to overaccommodative stress and defocus negative stimuli, wearing glasses with minus lenses causes your eyes to adjust toward counterbalancing/compensating for hyperopic defocus. (This also happens when a myope views near while wearing full negative correction.)
With the Power Vision System, the refractive (defocus) stimuli don’t happen by chance. Once aware of the effect of negative stimuli on your refractive ability, you should do your best to lessen the overaccommodative stress (either by wearing undercorrection or plus lenses), or you should work directly with myopic retinal defocus in the case of myopia.
Chance stimulation leads to slow adaptation, because the stimuli are directed without being aware of the reason. Being aware of stimulating our refractive system, as happens in the Power Vision System, lets us achieve positive results much faster, because the more we are aware of stimuli and induce them voluntarily, the more often they are repeated. At the same time, we should lessen and consciously avoid negative stimuli (overaccommodative stress). The sum of such stimulating leads to adaptation and consequently refractive change.
28. About the issue of restoring and improving the extrinsic ocular muscles’ coordination and central fixation/centralization, I’m following the Power Vision System and I’m getting much better:still 2 diopters per each eye, maybe at the moment just 1.5 thanks to the exercises you’ve proposed in your book.
I still have one problem I’m not able to resolve. When I look up, I notice that my right eye stops before the left one, and they don’t converge equally. Should I continue doing the exercises, looking up, till the extrinsic muscles around my right eye get relaxed, therefore becoming able to extend as much as the left eye’s muscles? Do you have any other exercise I can use for my right eye?
A healthy eye is perfectly able to point/fix at an observed object in all the parts of the visual field (both in the central parts and the extreme ones—as when you look up or aside as much as you can). Perfect ocular coordination is the result of the extrinsic ocular muscles’ perfect functioning. After being rehabilitated, from the point of view of functioning, through different specific exercises (rotation and movement), the oculomotor muscles also restore their flexibility, strength, and consequently coordination between the right and the left eye that allows your eyes to do the work that is required for correct focusing.
Don’t forget that a healthy eye has a capability of “vibrating,”which is characterized by saccadic movements and a pointing/fixating ability at all levels of ocular movement and in all parts of the visual field, including the peripheral ones, which are not used when wearing glasses. Even visibly, when observing healthy eyes, you can notice a different ability of viewing. The eyes that suffer from high myopia have an almost missing gaze, without fixing at anything: indeed it’s so, since myopes have a very low ability of achieving central fixation (some authors call this ability“ centralization”).
Centralization or central fixation is the ocular ability of making the image fall on the central fovea. If the extrinsic ocular muscles are not well coordinated (because of low strength and flexibility at the edges of visual field), just one or both eyes make the image converge and fall out of central fovea—on the yellow spot (macula lutea).
The phenomenon is called “retinal eccentricity”; it is also responsible for low focusing ability. When the eyes get back their ability of coordinating (and there are some exercises like ocular rotations and their variants that bring about better coordination), they will also be able to point and focus correctly on the central fovea again. Furthermore, the eyes will also start to vibrate perfectly again, having restored their normal saccadic movement.
Sometimes, certain anomalies in coordinating are possible during muscular rehabilitation through the exercises of rotation(especially in rotation fixing at a point). It’s necessary to restore perfect coordination, staying in the parts where you feel the “knots,” when the eyes aren’t able to maintain binocular fixation(fixing at a point while rotating), which results in double vision.
These results show the problem of coordination between the eyes as well as your ocular symmetry imbalance. Little by little, persist on rotating while fixing at a point in those parts of the visual field where you have some problems in coordinating/fixing, and you’ll notice better coordination/fixation and consequently better visual acuity.
The extrinsic ocular muscles are the striated type and, therefore, are subject to the same rules of “plasticity” and adaptation as any other striated muscle of our body (biceps, triceps). So, it’s necessary to train the ocular muscles according to one’s specific needs and then to go further with the exercises of retinal defocus, as described in the Power Vision System. Keep in mind: At first the
exercises apply for muscular rehabilitation (like rotations), and the exercises of retinal defocus come later (with or without training lenses). Before learning to run, your muscles must walk.
29. Is the Power Vision System based on any scientific elements? How did you figure it out? Please, let me know how and where could I get it. . . . I did some exercises with a therapist for two years, and I had some small improvements (from –5 to –2.5 D), but then I gave up practicing because I was fed up, and probably my sight got worse. I work at computer a lot and my job requires a lot of near-work.
The Power Vision System is based on physiological reactions like SAID (Specific Adaptation to the Imposed Demand) or retinal defocus, which have important and proven effects on the human body. The SAID Principle concerns gradual bodily adaptation to specifically induced stimuli, which leads to functional and structural changes in the treated organ—in this case, the eyes and the visual system.
The principle of retinal defocus concerns focusing-system compensation or adaptation to the induced stimulus: in the case of myopia a person is subjected to myopic defocus (becoming more myopic, lessening dioptric power of his lenses, or in case of middle/low myopia wearing positive training lenses). Such a phenomenon is called “fogging” and represents a “trigger”—the stimulus for retinal compensation. The training is aimed at using retinal defocus/fogging masterfully and specifically for each and every case of myopia/hyperopia.
The Power Vision System could also be considered a scientific method, since it’s based on physiological laws that are ascertained by traditional science. In addition, the effects of retinal defocus have been ascertained in studies on animals and especially in primates/monkeys.
If by scientific you are asking whether the Power Vision System was tested and the results were published in the journals on optometry, I can inform you that such tests haven’t been done yet. They are likely to be tested in humans soon.
A new scientific and experimental thesis is never born together with a series of studies and experiments proving it; otherwise it wouldn’t be new or experimental. This process of scientific understanding, and the results of scientific experiments, are described in Thomas Kuhn’s book, The Structure of Scientific Revolutions (1996;3rd ed.).
The Power Vision System has been written to explain and detail a system of treatment concerning both the physiological laws that it is based on as well as psychological phenomena beyond the visual system, such as bioenergetics. The system has worked in my case, but it’s up to each of us to check out its validity—taking upon ourselves the responsibility while being supervised by an oculist or an optometrist.
If you want to see whether this system works, you need to do the following: try to feel the effects of myopic retinal defocus without wearing contact lenses or glasses for half a day (you must be at a safe place, where you aren’t supposed to wear full correction for your personal or others’ safety). You are likely to notice or, at least, to have impressions of, better visual acuity at the end of the experiment: such improvement is a direct consequence of the visual system adapting to retinal defocus.
The Power Vision System acts directly and gradually, stimulating the visual system, getting used to and aiming at gradual regressing of functional visual error. Since the error is functional, the problem should be resolved by acting over working ability:this is the basis of visual reeducation.
You say you’re working at a computer, being obliged to view near, and you’ve also noticed that your sight has gotten worse after some positive results you achieved while working with your(very good) therapist. This phenomenon is due to the fact that you are constantly subjected to overaccommodative stress and constant visual axis’ converging (the latter needs the process of accommodation to act). If you want to keep all the positive results you have reached, you must allow your eyes to “space” over long distances. In doing so, the tonic accommodation will relax and the ocular axis will become parallel (eliminating the stimulus for converging).
As a preventive measure, you can also wear undercorrection (ora plus lens) when working at the computer. It is enough to wear undercorrection whenever you carry out near-distance activities or to lessen the accommodation through positive lenses. In the end, I would like to tell you that it works—really works! Certifications, diplomas, and scientific studies aren’t needed to ascertain something from our own experience. Work with the Power Vision System while being supervised by a physician, optometrist, or ophthalmologist.
30. Help! My sight is getting worse and worse. How could I avoid harming my sight for the rest of my life? I’ve been a myope for some years (0.25—0.50 D per each eye). Once I had perfect sight and I’m very sorry I can’t see as well as before. I study and work at the same time. Does this “work” somehow bring about my sight getting worse? I need clear, distinct sight for my job.
It’s very interesting to notice (and point out) your gradual development of almost all functional visual errors. If you ask anyone who suffers from a refractive error, he is likely to answer,“At the moment I wear –4 diopters, but at the beginning, my first pair of glasses was –0.75” referring to gradual dioptric power change in a negative direction.
Analyzing these simple answers, we can see that each person was changing her glasses constantly throughout the time due to her sight getting worse. It makes us wonder whether the “corrective procedure” works well from a therapeutic point of view, since in almost all cases it doesn’t cure the very problem at all, but even worse, it is contributing to the increase of overaccommodative/near-point stress. This results in decreasing focusing ability over time.
In recent years, medical science has made great steps and presently can treat a huge number of diseases and problems, but in this case of functional visual disorders we should wonder: What has been done for accommodative functional disorders like myopia, hyperopia, or astigmatism? Could we see the indiscriminate wearing of minus glasses and contact lenses as a therapeutic procedure?
Perhaps the present “treatments” for refractive errors should be checked out again from another point of view, which must be less “myopic,” knowing about the importance of the need for effective prevention. When someone’s leg is broken, the first step is to put it in a cast in order to heal the bone. Such a procedure is aimed at allowing the injured person to walk on his legs again. Sometimes he’s also given a pair of crutches to support his body weight and to make walking easier, until his leg is completely healed and the injured person is able to walk again. Keep in mind: The crutches are to be used until the leg is healed and walking is restored—but not beyond that point.
This does not happen in healing the sight by prescribing and wearing minus-lens glasses. Try to imagine a person who goes through a bad time and notices that his sight is getting worse. The person has a feeling of not being able to see well, and that what he could previously see is now blurry. Therefore, he looks for an ophthalmologist who diagnoses him as having low myopia and “heals” him with a pair of minus-lens glasses.
From this moment on, wearing such glasses, even at “near” where he doesn’t need them at all, this person’s refractive error will be getting worse and worse. A “functional error” is one that doesn’t act over the structure of an organ (organic disease) but over the way the organ is used—in this case, wearing minus glasses, or even worse, wearing full correction contact lenses(20/20—Snellen chart, per each eye) over time. When you do this, the visual system will become weak and tired (consequently, higher and higher dioptric power minus lenses will be needed).
In my view, this can’t be the right therapeutic procedure, since it doesn’t remove the initial cause of problem itself, but worsens it over time.
So, we shouldn’t be surprised when we notice that a person who wears full correction in almost all his ordinary activities demonstrates this myopic “propensity” and gradual sight worsening. This type of “minus-lens therapeutic” procedure for refractive errors degenerates the optically overcorrected person into an endless series of newer and stronger minus-lens glasses.
The result: Growing older, the refractive error will, most probably, grow.
The rule “Function makes the organ” doesn’t foresee any exception even in the case of visual organs; natural and physiological focusing ability becomes worse and is “ruined” by wearing full correction (minus glasses and contact lenses), as we do presently. Besides, such a procedure does not act on someone’s personal psychological, emotional, or other additional causes, nor on the stress itself.
Perhaps the reader is under too high overaccommodative stress(working and studying a lot). She might be under other kinds of stress at the same time (remember that the eyes suffer from emotional stress more than other organs), and all this has led to her sight going more negative. However, it could be healed in this initial phase simply by lessening the near-point/proximal stress (viewing in distance and, perhaps, wearing positive “leisure” glasses for all near-work). Besides, it would be very useful to have some break in your ordinary activities and to let yourself relax and rest. If you decide to wear positive lenses, it will reduce nearpoint stress and will improve distance focusing ability. However, you are to wear such plus lenses only when you don’t need full distant correction for safety reasons (for example, driving your car or doing a particular job).
31. I’ve been doing the exercises for over a year and half, looking for healing hyperopia in my left eye, blindfolding my right eye, and carrying out “slow” rotations with my left eye, as you recommended. I’ve got some positive results, but I don’t knowhow much my hyperopia has decreased (I started with about 4 diopters). Unfortunately, lately I haven’t noticed the same improvements as before. Shall I ever be able to eliminate my problem completely and have 20/20 sight? If I blindfold my right eye so as to make the left one work more, why do I need a lens to “worsen” my focusing?
Since there’s already a defect, I believe that the eye should try, by itself, to focus an image correctly until getting back to normal 20/20. That’s the reason I’m not able to understand what the lens is needed for, since it makes the image even more out of focus.
As for “the flashes of clear vision” you talk about, I have had just two of them, usually at night, and later on, I noticed a clear improvement. It happened some time ago and now—nothing, as if everything stopped, just a few, slight “stretching” feelings after doing rotations or after reading.
What does it mean? Has my eye reached its limit? Is there, perhaps, a problem in my brain, the part that is devoted to vision?
Since you are a hyperope, you must get your eye used to working at nearer and nearer distance. It’s a very slow and gradual process, but it’s sure and safe.
For example, if today you can read clearly at a 20-inch distance with your left eye (the right one is blindfolded), you must work on shortening this distance with time (reading at shorter and shorter distances).
When you are able to read at about a 4-inch distance, you can wear negative lenses so as to create an overload of fogging, which is suitable to achieve the adaptation.
In short:
1. Take a book.
2. Bring it closer till creating fogging.
3. Blink softly till you have a slight feeling of focusing.
4. Overcome this point of fogging/focusing, which creates an adaptation of your visual system. In your case, if you were once able to focus at the 20-inch distance, and now you read and focus at 12 inches, it means that your visual defect has decreased, since your eye has got used to the imposed visual conditions.
Retinal defocus is an optical stimulus that is artificially driven bylenses so as to ensure the adaptation of focusing. There are two different kinds of defocus: myopic and hyperopic. For myopic defocus for decreasing myopia (focal image is formed in front of the retina): Use positive lenses! Myopic defocus makes the eye become myopic instantaneously with positive lenses so as to ensure a certain decrease of overaccommodation. Hyperopic defocus, used for decreasing hyperopia (focal image is formed behind the retina), will use a negative lens. It allows us to increase the accommodation gradually with consequent decreasing of the hyperopia itself.
If you carry out the exercises of ocular stretching and gradually increase defocus, the adaptation and improvements will follow. The periods without improvements exist, and this is normal.
In such periods you must go on doing the exercises (especially increasing/ensuring defocus/fogging and adjusting). When you get to a critical point of imperceptible improvements, your focusing ability will undergo an adaptation, transient at the beginning, but later on, it will become steady.
Scientific studies in animals have proved the effects of retinal defocus on changing your refractive status. The animals, which were subjected to different kinds and levels of defocus, demonstrated the eye’s adaptation toward either myopia or hyperopia.
When you stop training your eyes with defocus (specific for your refractive error), you will also stop having any improvement. If a hyperope goes on doing the exercises of hyperopic defocus, correctly and continuously, he is even likely to develop the opposite error—myopia. On the other hand, a myope who is trained with myopic defocus theoretically could develop hyperopia unless he stops training at the moment when he reaches the emmetropic state. The rule is to use the state of retinal defocus till you reach the awaited level of adjustment (therefore the improvement).
The eyes, as well as the sight, are influenced by your emotional and mental state. It is a very interesting and important issue, since working on our eyes, we also intervene over the blocks and emotional processes that are at the base of the defect itself. The relation between refractive errors and some kinds of characters is well known: a myope is mostly an introverted person, as if he were closed into his own world of narrow vision, within the limits of ability to focus.
A hyperope, on the contrary, is a person who turns his attention “outside,” as if there were a danger to avoid—his sight and his inner world are directed toward the distance. There are as many kinds of characters as there are people: we could say that the character represents a kind of “imprinting” that reveals itself through the eyes. Psychotherapeutic techniques, like EMDR (Eye Movement Desensitization and Reprocessing) and EMT (Eye Movement Technique) work on ocular movements so as to resolve emotional conditions and trauma that influence the patient. Here, we can see the direct connection between the eyes, brain, and sight. According to the same neurolinguistic planing, different parts of the eyes have a certain, direct influence on the brain: looking up toward the left stimulates some parts of the brain in a completely different way from when looking down toward the right.
It’s interesting that by working on our sight we can influence and modify our own capability of inner perception as well as dealing with the surrounding world.
Different levels of refraction can make us able to either move away from the surrounding world (though fogging) or to embrace it with our sight—and also with our emotions. Body, mind, and soul are the mirrors that reflect our own light into one single mix—which represents the person with all his characteristics. So, we can state that the techniques of working on the eyes have avery strong component for transforming the person. The eyes are the filters for our surrounding world: change them and your perception will be changed, as well as your being and capability of dealing with others.
32. I wear correcting lenses (undercorrection) and my sight is blurred when I view distances! What do you advise me to do?
The fact that you are in a perpetual state of overaccommodation(wearing lenses with full correction and viewing near, as it happens almost always indoors, leads you to your viewing over 20/20). This condition ruins and makes the natural focusing become lazy. The fact that you are not able to see perfectly in distance is the first step of visual reeducation; the goal is to stimulate the natural capabilities of your eyes—but not of the lenses. PVS foresees, in its second phase—retinal defocus (to increase visual acuity)—making the eyes become transiently myopic, so as to stimulate an adaptation of visual system (it may happen with or without training lenses).
It is important thing to follow the techniques the right way.
33. I’m going to put some questions to you about carrying out the techniques, so as to be able to start practicing.
a. Concerning the exercise of stretching “rotations fixing at a point,”am I supposed to turn my head on a horizontal level, fixing at a point (as if I were shaking my head, No), or should I carry out an imaginary circle with my head, fixing at a point?
b. Which exercise is the most important, “rotations fixing at a point” or “cyclorotations”?
c. In the Basic Level Program, are you talking about rotations with open eyes (stretching variant for rotations fixing at a point) fixing at a point at over 10 feet of distance, or about those that are described as a “stretching variant for cyclorotations,” as if we wanted to follow the borders of a very big clock? If the latter is the right one, how could I fix at a point if I’m carrying out rotations with my eyes?
d. As for stretching in the static position, but not the circular one:For how long am I supposed to keep a certain position? Maybe I shouldn’t stay still in one position but alternate with certain rhythm and speed?
e. As for taking breaks while working on reading with positive training lenses: For how long am I supposed to read before having a break? For how long should each break last? Am I supposed to take off the training glasses during these breaks?
f. Is the size of the letters in the text very important when we train to read with training lenses? Which size is the best one?
g. Is it true that some people are able to reach visual acuity over 20/20 with the methods of visual reeducation?
h. As for different acuity between two eyes: Which difference (in diopters, if possible) requires training with reading with suitable lenses on, blindfolding the weak eye at first, so as to make it equal to the good one? When isn’t such a difference important?
i. If I understood well, in training with training lenses, the true reading of the text starts after focusing it perfectly with CRB movements, and only at that point should we read it, as long as it’s perfectly clear; when the text starts becoming blurred again I must repeat CRB movements and then start reading it again. Or, if after CRB movements the text is still slightly blurred am I supposed to read it?
j. Here’s a paper with the image of three lines of the text that I gradually made blurred. Can you tell me which one among these lines is to be considered an initial level of fogging of the text to be followed with CRB movements?
Here are my answers:
a. The exercise of ocular stretching “rotations fixing at a point” must be carried out so as to let all the extraocular muscles be subjected to the same level of stretching out. If you carried out this exercise only on a horizontal level (as if you were shaking your head, No), you would work only on symmetry and coordination of your “right and left” musculus rectus, butnot the “superior and inferior” ones, as would happen even nodding Yes with your head. “Diagonal” positions must betaken into account.
b. The importance is to be attributed to the level of efficiency. The exercise of “rotations fixing at a point” is more efficient than simple rotations because we directly act over symmetry and coordination between both eyes. Probably, it’s very hard to keep “fusion” between the eyes in some extreme parts of the visual field: such a condition shows an imbalance between strength and flexibility of the two eyes. The consequence of such imbalance is a low binocular fixation on one side, and on the other, the lower level of “central fixation” or “centralization.” Any shifting from the central fovea leads to a lower quality image. This is the reason why ocular stretching is particularly beneficial for restoring your visual acuity.
c. You can fix at a point, carrying out the rotations with your eyes and keep on fixing at a point at the same time.
d. In the positions of stretching, the time of keeping each single static position itself determines the level of intensity of the exercise: the more you maintain one position, the more intense the exercise will be and, consequently, the level of muscular contraction (agonist) as well as the level of stretching out and lengthening the muscle that is antagonist to the movement. The duration of fixing is approximate and it must be adapted to the initial strength and flexibility of the ocular muscles. The duration must be adapted and lengthened little by little, until the muscle gets used to the load, or the intensity (the relationship of ocular range/duration of contraction). Like in the exercise of retinal defocus, if you don’t increase the training stimulus gradually, the adaptation and consequently the improvement in visual acuity would stop.
e. The duration of the breaks is approximate and must be adapted to each person, so trust your feelings. As soon as you feel ready, go on doing the exercises of retinal defocus. I advise you to take the training glasses off during the breaks.
f. There’s no perfect size: the basic factor is to create slight fogging, to make the text become slightly blurred, trying to focus the letters.
g. What is usually called “emmetropia” is a simple convention:such convention is still at 20/20 visual acuity, according to the Snellen table. Monkeys, and generally all wild animals, have more or less clear levels of “hyperopia,” as it would be defined concerning this “convention.” We could develop the visual acuity over 20/20 with PVS. If man had stayed wild, without being constantly exposed to the state of overaccommodation due to narrow places (indoors), probably 21/20 or even more would have been considered as normal visual acuity. The way to run so as to overcome 20/20 is the same one that the myope must run to recover from his refractive error. The exercises are the same: muscular training and retinal defocus. The only difference is that a myope works with low positive lenses (for example, +1), but the person who wants to overcome 20/20 must ensure a suitable state of retinal defocus with +8 diopters. It’s important to increase visual-acuity viewing in distance and maintain it in viewing near; otherwise we run the risk ofdeveloping hyperopia (farsightedness with little adjustment at near distance). It’s up to every single person to see when is the right moment to finish working with defocus.
h. We shouldn’t care a lot when the difference in adjusting/focusing between two eyes (anisometry) is 0.25. If it is higher, at first, we should work on the weaker eye (which suffers from
a greater visual defect) to take it to the same level as the other one. You can work on both of your eyes at the same time.
i. You have understood everything completely well: the work you carry out must be with slight fogging (moving the text away or bringing it nearer; it depends whether it’s a matter of myopia or hyperopia), the CRB movements, focusing. Then repeat thesequence.
j. The higher the level of fogging with which you are able to focus well, the higher the level of adaptation and consequently the improvement for your eyes. For fogging as in number 3 in your image, adjust with CRB movements until the image is more in focus, like number 1. Then, repeat the sequence, if possible, moving the text away.
34. Before starting to do the exercises, I have a few questions. Am I supposed to start training with focusing after having trained my ocular muscles for some time (days? weeks? months?) or should I start doing both at the same time? I wear correcting glasses for myopes with 4.5 D lens on my right eye and 4.0 D on the left one. In a training session without my glasses (I hold a book at about a 12-inch distance), only my less myopic eye (the left one) works. Should I train with focusing, putting additional positive lenses over my correcting glasses so as to make both my eyes work, or should I train without my glasses, blindfolding my right eye till it reaches the same level of myopia as my left eye?
Every myopic person has stiff and inflexible extrinsic ocular muscles, due either to misusing or not using them. Misuse means both abuse in wearing glasses (for example, at near distance where adjustment is possible even without lenses) and wearing glasses when you don’t really need them at all, in “safe” places—at your home.
“Preliminary” work—before starting training with retinal defocus—with or without lenses is needed, because those stiff and poorly flexible muscles penalize all your work with retinal defocus, jeopardizing your improvements. Purely “muscular” preliminary work (the active stretching as described in PVS) allows you to have better results in training with retinal defocus since the muscles become more able to relax and focus.
Another great advantage of the preliminary work is the result of restoring the right ocular muscles’ symmetry: correcting “wrong” positions that over time will lead to adaptations of the ocular muscles, which may even lose their symmetry (equal relationship between strength/flexibility of all six ocular muscles). The quality of adjustment depends additionally on the capability of central fixation/centralization (the capability of adjusting or “pointing” the image on the central fovea). This work is aimed at restoring the capability of centralization/central fixation and better muscular symmetry. This can give only “visible” advantages, above all when focusing in the presence of retinal defocus (carrying out the second phase of the PVS program).
Even though the retinal defocus technique isn’t widespread, it would be wrong to state that it doesn’t exist or that it is inefficient. Your eyes will show it to you after you have carried out the specific training with retinal defocus for some time.
When should you start working with retinal defocus? The very same rule of common sense works here: always follow the principle of retinal defocus.
There’s no standard time before starting to train with defocus. However, you should start with the first phase of PVS, carrying out active stretching with your oculomotor muscles and making them work at a maximum range of the visual field.
I advise you to work, at first, with retinal defocus on your “weaker” eye. You can do it by blindfolding your “better” eye and training with retinal defocus on the other eye until both eyes are at an equal refractive level. At that time you can start working with retinal defocus with both eyes.
35. I work as a dental technician and I would like to know whether my job environment may jeopardize my sight recovery, doing the exercises.
The answer is Yes. One’s job environment as well as the life one leads acts on our refractive state, since we get used to our visual environment. Constant near-work can make focusing at a near distance (the process of accommodation) “become chronic,”staying in such a state even when accommodation isn’t needed—as when viewing in distance (at infinite distance).
Such near-work conditions, over time, may lead to a “spasm of accommodation,” where the ciliary muscle is in a state of chronic contraction, thus creating pseudomyopia or transient myopia.
Over time it usually gets worse and steady (it becomes an axial lengthening of the ocular globe). This result has its equivalent physiological explanation and is one of the ascertained causes for myopia development: a prolonged state of hyperopic defocus. According to the theory of defocus, the retina is subjected to repeated adaptations, depending on the position of focus. This simply means that the eye acts as a camera with an autofocusing system, constantly varying focus according to the distance of the observed object and therefore the position of focus—the position of the image on the retina.
According to the theory of retinal defocus, the condition of constantly maintaining the focus behind the retina, over time,
creates axial myopia, with the consequent lengthening of the ocular globe. This is the characteristic result of medium and high myopia. Such axial lengthening is the result of retinal adaptation(and eye length) to one excessively confined—in time and proximity—to that “near” environment.
Accepting this theory as the accurate one, the opposite can work as well: if the focus is maintained in front of the retina (creating
myopic defocus instead of the hyperopic one), the retina will constantly be trying to modify the focal level to the focal point, consequently stimulating the relaxation of accommodation that leads to better visual acuity and decreased myopia.
One of the principles of visual reeducation in the Power Vision System is based on this theory: using suitable retinal defocus we can lead the eye to adapt its refractive ability and decrease the
initial refractive error until, possibly, compensating for the error. Such results have been obtained in experiments in many animals that were subjected to different states of retinal defocus.
Coming back to your question: one’s refractive ability directly depends on the quantity and the kind of optical stimuli she’s subjected to, either at near or in distance. According to the theory of accommodative balance, if the near-distance stimuli prevail, they may lead to myopia development.
There are two solutions for this problem:
1. Lessen (or eliminate) near-distance stimuli (changing the type of work with one that allows you to space your sight). This obviously isn’t an acceptable solution.
2. Don’t let your eyes be subjected to overaccommodative stress, even though you are carrying out near-work. You can obtain the latter result simply by wearing positive lenses whenever carrying out near-work. The process of accommodation has positive effects on focusing at near distance, allowing better focusing ability and visual acuity. Wearing positive lenses in near-distance activities, you can prevent your eyes from excessive near stimuli. This is a great protection against developing myopia.
The dioptric power of the lenses is to be calculated according to one’s refractive error and personal needs. An oculist or an optometrist should prescribe the right lens dioptric power.
36. I’m a myope, –6 and –7 D and 1.25 astigmatism per each eye. Shouldn’t I let the muscles that are responsible for adjustment go? I feel as if I have blocked them. I think that using body-building methods, which worked well in your case, wouldn’t be useful for me. Perhaps they could even be dangerous. My eyes see as they like and they can’t be manipulated like biceps muscles. When training to visualize an object, I’m not able to keep it still and fixed in my mind: it goes away, escapes, runs around my mind, and doesn’t let itself be observed in all its details. The same thing happens with my myopia. Whatever I do, it’s as if it were completely useless, as if it were to pay for my impatient ego, which has always been looking to cancel my unconscious part and all the processes in my body. Please, in your opinion, how could I improve my visualization, speaking in psychological terms? What do you think about my relationship with my mental images and how could I, gently, lead them to fixation?
You do not need to understand the psychological bases of your myopia, nor the reasons for your impatient ego, to be able to myopic people improve your ability of focusing. In your case, just being willing to understand could be a symbol and the proof of a much too analytic personality—“brain type”—that is characteristic of myopic people who tend to “make a concept” of everything. Despite very strong psychological components that are hidden behind every visual and bodily process (as proved in psychosomatic medicine), it isn’t the most important thing. You don’t need to psychoanalyze yourself to resolve or lessen your problem.
You don’t have to analyze the image in front of your eyes so as to see it; the only thing you have to do is to simply let the image pass through your eyes. You must work on visual rehabilitation very hard, train and do the exercises, without having psychotherapy.
A normal capability of focusing requests “dynamic relaxation” of the extrinsic ocular muscles, and (as you say) “you should let them go.” But how to do it and how to let them relax from chronic tension, which blocks their natural capability of “saccadic vibrating” and “central fixation/centralization”? A famous school proposes more or less specific exercises of “relaxation.” From my long, personal experience and in my opinion, simple muscular relaxation isn’t enough to alleviate completely the chronic muscular tension of an overcontracted muscle. It is necessary to restore the physiological muscular qualities like
strength and flexibility.
In such a sense, you can train doing the exercises of pure muscular work like active static stretching: simple, but very efficacious exercises for decreasing muscular tension and for better centralization.
In this first phase of pure muscular work (you don’t have togo to the gym to do the exercises), you must work with suitable retinal defocus, with or without lenses on (suitable means that the level of defocus must be calculated on the basis of your own refractive error).
Little by little, as long as your sight is being improved (if you do the exercises constantly and with perseverance), all that’s psychological and beyond your myopia will be gradually restored. Then you will probably see that your capability of visualizing is getting better, as well as your memory, and (as it happened to me) also your dealing with people. Additionally, you will trust in life and in the power of self-healing much more.
37. I’m almost thirty-two and I’ve been living with myopia ever since I was fourteen. The problem is that I’ve grown up, but my refractive error is still increasing, very slowly. In all these years everybody has thought that my myopia is a genetic condition and can’t be stopped. (I’ve seen many ophthalmologists and university professors, read books on ophthalmology, and I hope I’ll take my degree in medicine very soon.) At this point, I can’t do anything else but hope that all these ophthalmologists could be denied. It’s true (as you know it well, since you study medicine) that it’s very hard to overcome the theories and scientific dogmas in any field—especially in the medical one. Who would dare to question an already accepted theory? Now, too many previous certainties are questioned and the standard mantra about genetics is wearing thin. With time, then, the box-camera theory will collapse because of all the evidence against it. This book is about results that people can have by daring to overcome such obsolete paradigms. This means healing and recovering their distance vision to normal by clearing their refractive errors. Science must always evolve but never become blind and imprison itself, unless it wants to run the risk of becoming obsolete by its own dogmas. True science should always question methods that have been handed down to us by a traditional quick-fix philosophy. Nowadays society is more interested in putting on correcting glasses than in allowing people to know the truth about their eyes.
The answer, of course, is up to you—after reading the book. You’ll carefully study the PVS physiological bases, and above all else (you should be constant in doing the exercises), you’ll have a chance to see the results with your own eyes.
I hope you’ll take a specialization in ophthalmology: probably you’ll become a pioneer in the field, having read and learned all that is written about the Power Vision System.
39. I’ve identified three people who seem to be interested and motivated to carry out the Power Vision visual rehabilitation program. All three cases have the following training schedule:Ocular stretching three days per week, three times per day, wearing positive +2.50 lenses on each eye in all activities that allow it (reading, working at computer).
a. Marco (my son): –6.25 right eye (RE) –5.50 left eye (LE) (asymmetry due to keratoconus). After having trained for four weeks, now he usually wears –5.50 RE and –4.75 LE and according to Snellen tables he has full sight now, even though after working(viewing within 10 feet distance) he notices some worsening. He is the only one who doesn’t do any exercise regarding fogging/retinal defocus.
b. Francesca: –1.25 RE and –0.75 LE. Next Sunday she’ll finish her first week of training. Her schedule includes also the exercises of defocus/focusing.
c. Massimo –2.00 per each eye. Same story as Francesca’s.
My questions:
a. Does the method change depending on age?
b. Should I correct the training schedules of my three samples?
c. When is the right time to change the additional lenses? Should they stay the same? Should both myopes and hyperopes always wear the additional lenses in near viewing (a kind of everlasting visual hygiene)?
d. Marco has told me that he feels better (and sees better) wearing his present glasses. When is the right time to change graduation for distant viewing?
Entire ocular capabilities must be used so as to maintain ocular strength, flexibility, and coordination correctly. It can’t happen if the sight and its capabilities are imprisoned within a limited visual field, as happens when we view through the framework of our glasses.
Regarding the use of positive +2.5 D lenses, I must warn you that the defocus state is to be modulated and changed masterfully, depending on each type of refractive error and, above all, depending on the entity of the error itself. A –0.50 myope can use and wear positive +1.00 or +2.00 lenses when he carries out neardistant activities (so as to oppose the level of overaccommodationthat has come from viewing too-near targets). In the case of highermyopia (for example, 2 D), the accommodative state should be limited by taking off the glasses (if it’s a case of medium myopia); it’s also useful to decrease the lens dioptric power for distance viewing (negative lenses). A myope like Marco (rather high myopia)should wear undercorrection in near viewing (decrease the lens power for some diopters), or, at least, he could carry out his near-distance activities wearing his present lenses and wearing the positive additional ones (for example, a pair of –6.00 D glasses and another pair of +2.00) over the first ones. In this way he decreases the accommodation and dioptric power at –4.00 D.
The use of retinal defocus and therefore the level of the imposed defocus must be changed depending on aim: low positive lenses are to be worn so as to prevent myopia (to decrease an overaccommodative state), but for decreasing myopia gradually you must work with a higher defocus level, which couldn’t be used in ordinary activities without jeopardizing visual acuity. The defocus stimulus is aimed at stimulating a compensation for the error as well as at increasing refractive capability, and that’s why it must be temporary and limited to training sessions.
To answer your questions:
a. The results differ not so much depending on someone’s age as on the time she’s been wearing glasses (for how long a time her focusing has been “frozen” and helped with lenses, causing “disuse” or functional atrophy due to misuse).
b. It’s okay to carry out ocular stretching exercises three days per week and three times per day, but you should make your “samples” understand that muscular work at maximum ocular range must become their ordinary viewing. That’s why they must acquire the healthy habit of short ocular rotations while relaxing in the morning, like while brushing their teeth. Keep insisting on the exercises of ocular stretching, fixing at a steady point and at the extreme parts of the visual field. Do your best to make your “samples” carry out the exercises correctly, gradually increasing the rotation width and staying on the parts of the visual field where the work is very hard, due to “blocks” (at those places where muscular strength, flexibility, and coordination are limited).
c. The defocus state must be changed, increasing the dioptric power of positive training lenses, when one can read a text or letters holding the text in completely extended arms and wearing training lenses. In such a case it would be impossible to work with defocus unless increasing the training lens dioptric power.
As long as we are chronically subjected to overaccommodative stress (near-point stress) without counterbalancing it with distant viewing, it will be necessary to use positive lenses for the purpose of prevention and maintenance. Even only 1 diopter positive “leisure” lenses can prevent myopia development, when we become emmetropes.
d. The graduation for distance vision is changed depending on one’s present refractive capability and needs. Some ophthalmologists and optometrists prescribe low undercorrection. However, the limit depends on the person’s needs: if you are a driver or pilot or someone whose work requires perfect sight, you must wear full correction. If not, undercorrection works well, wearing it only when necessary for clear vision. Many people wear their glasses (or even worse, contact lenses) even when they can see clearly without them. Such a situation does nothing but worsen the accommodative balance and allow the state of chronic overaccommodation, leading to ever-higher refractive error.
41. I’m twenty-three and I gave up wearing my glasses when I was eighteen, looking to improve my sight. At that time, my diopter (I was a myope) was just 1 D per each eye with a low astigmatism in my left eye.
I’m in a much worse situation today! I can hardly go around without my glasses, though I haven’t worn them for over five years. The last time I went to the ophthalmologist, I had –2.25 in my right eye and –1.75 in the left one. It’s surely much worse today.
I discovered your method, and ever since then I’ve realized that my sight is getting worse and worse. The first three years without wearing my glasses I was able to keep my myopia almost shifting
whenever I could, and, despite everything, my myopia was low. Now I go to the university and follow your advice. I always study holding the text as far as I can, even though I must read more slowly; I do ocular stretching in front of mirror every second day, and I do my best to view distant whenever I can. I never put my glasses on, only my contact lenses (undercorrection), and only when I play football (three or four times a week).
The day after doing stretching exercises, I see less, my eyes are stiff. And when I do stretching I’m not able to notice any block or knot. I’m doing it as best as I can.
I gave up doing the exercises of defocus with positive lenses +1.00 because my sight wasn’t clear the day after doing them. Last year, as soon as I took off my +1.00 glasses I had some clear “pulling,”but not anymore. Now I only do defocus without positive lenses, but the result is that my eyes are even more stiff.
I have the feeling that whatever I see is a bit blurred, and my eyes are as hard as crystal. Doing stretching exercises, this feeling gets even greater.
Could this theory of mine be true, that my eyes are getting used to sighting everything and are always blurred? Defocus stimulus doesn’t do anything but make me get used to the blur even more.
Since I’m a student I study a lot, even if at the furthest possible distance. Could you suggest an optimal program, perhaps one exercise, even if it is difficult and takes a long time to do? (I can find an hour or two a day.)
Figure Q.1 shows the relationship between recovery time and muscular performance quality increase—in this case muscular strength increase. After being trained, a muscle suffers from physiological performance drop, and later on, with time, it overcomes its initial performance limits (strength increase).
Figure Q.1. Relationship between Recovery Time and Muscular Performance
If recovery time is short (as in your case; see also points 1 and 2 in Figure Q.1), the muscle has no time to “overcompensate” and become adapted or increase its strength (overcome the horizontal level of its initial performance).
If recovery time is long enough, you can obtain the necessary adaptation (point 3 in Figure Q.1 in the case of ocular muscles). If recovery time between training sessions of ocular stretching isn’t long enough, the result will be a transient and physiological worsening of saccadic vibration and focusing.
If I were you, I would recover much longer, doing the exercises of ocular stretching with two days recovery time at least. The recovery factor is a very personal one and it depends on one’s physiological qualities. The training rules regarding ocular muscles are not different from those for any other bodily muscle: both kind of muscles are the striated type and therefore can be trained voluntarily.
So, train but don’t forget that any increase in muscular capabilities(even focusing) also depends on the right recovery time and not only on factor of training itself.
42. I often take a bicycle and ride away, go to the seaside or river to view, observe, and discover what I really see . . . what I’m able to see with my own eyes. In my opinion my sight is a dynamic phenomenon and there’s nothing static in it. I have some flashes of clear vision, and the distance at which I’m still able to see clearly is changing every moment. The indoors isn’t good for restoring my myopia . . . even though I believe it’s not the only reason.
One’s refractive capabilities depend on many different factors like physiological, mental, emotional, or environmental ones. Having understood all the eye’s capabilities of getting used to the induced stimuli—both the near and the distant ones—you can intervene over ocular focusing capability effectively and voluntarily. The refractive state depends on the balance between near and distant stimuli.
The awareness that focusing power is a dynamic phenomenon is the first step toward healing. No human organ nor bodily system makes an exception: when an organ (heart, lungs) undergoes the right stimuli it is pushed toward adaptation. Why should the eyes or refractive system/focusing be an exception?
Do the exercises of ocular stretching and retinal defocus and let me know about your improvements!
43. I’ve been doing the exercises from your Power Vision System for two months, because I have very high myopia. I am able to focus on text perfectly, doing CRB movements, and now I hold it at a5-inch distance (at first it was 6 inches)! Some days ago I thought I could carry out CRB movement while viewing the landscape(houses, streets, people), and I was able to make my vision clearer and sharper. Now I’m able to distinguish even distant targets and read license plates and registration numbers, billboards, traffic signs—all that was a dense fog before. Yesterday, doing CRB movements, I was able to see perfectly each single rock on the mountain behind my home.
Is all this dangerous for my eyes? Can I go on or I should restrict myself to only train by reading a text?
I’m very glad that you’ve put the PVS program into practice. Since you’ve noticed the first improvements and as your refractive capability changes, depending on the specific imposed stimuli, the next step is to keep doing the exercises. It’s very important to adapt the training load on the base of already obtained improvement. Load, in this case, means the capability of focusing the low state of blur/fogging at ever further distance(for myopia). Load also means the relationship between the lens power and the reading distance. There’s no contraindication for carrying out CRB movements even for distant targets (license plates, billboards), but it is a procedure aimed at restoring the right ocular relaxation, which is necessary for correct focusing. When all the steps of your improvements become stable, you won’t need to carry out such a procedure, and you’ll be able to see without any effort or will. It’s true that CRB movements let you learn how to focus distant targets voluntarily, but the final goal is to make the sight be what it really is: a natural and spontaneous ocular capability.
44. A year ago I underwent PRK surgery in both eyes as to correct 7 D myopia and astigmatism. Now, a year later, I’m still a myope—about 1 D on my right eye (which has always seen less than the dominant left one). After the analysis (corneal topography, and soon), we understood that my myopia is the accommodative type. With my surgeon’s approval, about three months ago, I started training five days a week, with positive lenses only on my right eye (+1, +1.25, +1.50). In the beginning I hardly read 3/10 on Snellen tables. Now, though it isn’t easy, I get 9/10. In spite of these very good results, my right eye vision is still unclear. Am I doing everything correctly?
I think that your results speak for themselves. 6/10 improvement in three months is a more than great result, even if your last improvement isn’t stable yet.
Passing from +1 to +1.25 and then to +1.50, you’ve respected load/stimulus increase, the gradual retinal defocus increasing with lenses through the CRB system. You’ve got the response of your refractive capability and consequently better focusing. I think you were very lucky because after laser surgery your myopia is still the “accommodative” type. In the opposite case (if your cornea were deformed), the Power Vision System wouldn’t help you at all since it acts over extrinsic ocular muscles, the state of tonic accommodation of the ciliary muscle, and the level of central fixation, but not over corneal geometry and its curving. If the surface of a camera lens is damaged, it is useless to work on the focusing system; it’s necessary to repair the lens itself. Since your lens, your cornea after corneal topography, is still good, you can obviously intervene over the focusing system directly, as any other person would.
Keep going this way, which has brought you a 6/10 improvement in three months, and keep going, giving a constant increase of defocus in the eye that needs it. Keep going this way as long as your focusing capability is being increased (when necessary, pass to +2, +2.25).
Any adaptation always follows a gradual stimulation. Listen to your ophthalmologist’s advice. She knows everything about your case and can make the right medical diagnosis.
45. I wear +1.25 lenses at the office (I should correct 1 D) for two hours a day, all week long. Is it reasonable to wear +1 glasses at home, even without reading, and for how long should I do it?As long as the eyes are subjected to near-point stress, it’s reasonable to do our best to mitigate overaccommodative stress, wearing low undercorrection, or, if necessary, positive lenses (for myopia).
All the activities that require near vision (like reading, writing, working at a computer, or any other kind of indoor work) contribute to such stress. The use of positive “leisure” lenses (in the case of myopia) should be limited to two cases:
a. To prevent myopia that hasn’t shown up yet. In this way we can (optically) shift the focal point with lenses, eliminating or mitigating overaccommodative stress (near-point stress).
b. Leisure lenses for stable myopia. We can use them together with(but they cannot replace) ocular stretching or retinal defocus.
As far as I know there’s no contraindication for wearing low positive lenses (for low myopia) and low undercorrection for high myopia, indoors and at any other “safe” place (like home). However, when using lenses, a person must consider his own and others’ personal safety as well as any possible danger that could come out of slightly blurred vision.
46. I’m a researcher and I work in Italy, but I also collaborate with some American and Australian universities. Our research deals with experimenting with new treatments for ocular disease and refractive errors. I’ve been working in a team for over ten years and we’ve been holding congresses worldwide for over thirty years. Every day hundreds of scientists, who know outer and inner ocular structure better than their own pockets, are discovering new techniques that could contribute toward healing ocular pathologies and visual errors.
We have explored your site very carefully and, at least in the beginning, we were very interested in it, but later on our interest changed into amusement. With time even amusement faded away and was replaced with moral worry.
Only scientists (as we are) can understand that the false promises of “your technique” are aimed only at selling your “magic” book. I would like to let you know that thousands of desperate people would follow anywhere a prophet who preaches curative formulas(which are indecent from a scientific point of view) to resolve their problems.
First, thank you for your e-mail. I’m very sorry I caused amusement among you—the people who work in the ophthalmologic sector—and furthermore, I’m sorry I was your “moral worry.” All that I learned, I did because of the great (unfortunately)ignorance that reigns over refractive errors. Let me add something else: if a “moral worry” must exist, I would look for it in the million-dollar business in glasses, contact lenses, and refractive surgery.
I would like you and your team to give me more solid criticism on what I wrote on my site. I think you should see what I state in my book. I’ll personally send you a copy.
I accept any criticism, as long as it’s based on scientific facts and reasoning, but not simply saying “You can’t.” Only ophthalmology is considered a “closed science”: we have been working with the same assumptions for over a hundred years. The first of them is that ocular structure is “fixed,” like a camera’s, and that it doesn’t change depending on someone’s visual environment.
One theory on axial myopia (a deformation of the ocular globe)shows that with time, such a deformation (the retina itself) shifts, looking for the right focal point.
I’m sorry that you and your staff see me as a kind of “enemy.” It would be much better to weigh thoroughly all that I wrote and experimented on my own eyes, reading my book carefully, examining what I state, and comparing it to scientific deductions. Each of my statements is backed up (as much as I could do so)with scientific works of international value. They are listed in the References.
Changing one’s accommodative balance, the average of visual stimuli one gets every day (manipulating his visual environment optically), we can also change his refractive state: at first temporarily, and then summing up all the little adaptations, we can get more stable variations. This happens to myopes when doing the exercises of “disaccommodation” with positive lenses and undercorrected glasses, artificially creating a myopic defocus.
I would like you and your staff not to see me as “a visionary without morals” but as someone who is keen on sight and has spent thousands of hours of his own time studying scientific works. Moreover, I undertook this with my own money, without scholarships or being sponsored by companies that take part in selling or the “business of sight” (as often happens with “worldwide congresses” that are sponsored by such companies). Now, let me ask you something: How much independent judgment is granted to the real and scientific possibility of preventing and of curing myopia, if such congresses are based on and sponsored by “technical sponsors” that are interested in selling, and therefore are not interested in anything that releases consumers from buying glasses, contact lenses, or refractive surgery?
If I threw dust in the blind’s eyes I would deserve to become blind myself. On the other hand, if I kept silent on all that I’ve learned, I would be a partner and ally in a vision business like the current one.
I’m at your complete disposal for any further explanation you need.
48. I have several questions for you.
a. Myopia is due to excessive ocular bulb elongation. Therefore, it means that one who improves his sight should have ocular bulb shortening. Has anyone checked it out?
b. I have another question for you: Is there any limit concerning the level of myopia that could be cured (perhaps due to the highest level of ocular bulb elasticity that can’t be overcome)? Let me explain it better: myopes who practice the exercises reach some improvements that are limited to 1–2 diopters. Does it mean that it is impossible to heal myopia completely if it is higher than these values?
c. When I carry out rotation with my head, I have double vision in two points. There’s no binocular focusing. . . . What should I do?
d. Should the ocular relaxation in CRB be simultaneous with blinking, or just follow it?
e. For rotations at extreme points: does it mean that fixing at a steady point at 10-feet distance, the head must rotate while bending downward and then upward, very slowly carry out such movements over and over again, and maintain binocular vision? But. . . my nose hinders binocular vision in lateral zones. So, what should I do?
f. Do you have the phone number of any ophthalmologist or ocular therapist who approves and uses ocular gymnastics?
Let me answer your questions:
a. Ocular bulb elongating (axial myopia) happens after longlasting retinal defocus (near-point stress, overuse of lenses and glasses, excessive nervous stress, bad nutrition, and so on). Only after some time, transient myopia or pseudomyopia becomes an axial deformation of the ocular bulb. The very same thing works also in the opposite way: it takes time, and after sometime all the improvements (due to practicing) can improve the ocular bulb form (better focusing, ocular movements, less ocular tiredness). We are in an experimental field (even though the causes of elongation are acknowledged by science as well as tested). My advice is, Practice the exercises without conjecturing too much—you don’t need it for good results. The will to learn is an advantage, but on the other side, if you stop and conjecture, then it is a disadvantage. What is really important in the Power Vision System is practicing, after arranging the exercises depending on your needs (refractive errors, muscular imbalance, retinal defocus entity, the choice of correcting lenses[full correction or undercorrection]).
b. The highest myopia to be cured doesn’t exist, nor does the highest theoretical level of myopia development, except the limit of retinal breaking due to excessive axial elongation of the ocular bulb (the latter is another reason to start doing something more for your eyes and your myopia besides the palliatives of wearing glasses, contact lenses, and refractive surgery). As for the latter point, refractive surgery itself: After undergoing refractive surgery, no eye is healthy, despite its ability to focus, because the ocular bulb deformation persists. Furthermore, such deformation can worsen into retinal detachment, with time, and if “myopizating” conditions come back. Either refractive surgery or the Power Vision System takes a long
time to see complete improvement. Out of 500 people who learn about PVS, 200 of them practice only during the first month, and only 100 carry out the whole program with perseverance till the first results, and only about 50 of them get further results, which come with time. Not all of the latter group are willing and able to link up to the Internet to share their results with others. Unfortunately, we don’t have follow-up studies to monitor all the patients throughout time; therefore, at the moment, the results are anecdotal, but not unreliable. With time, as the technique spreads out, more and more voices will be supporting PVS visual rehabilitation. In the meantime, this technique’s “pioneers” can be the first to overcome the limits of myopia that are imposed by present medical science (and not by scientific experimentation, which has been affirming the refractive state dynamism and changeability for a long time).
These “pioneers” will experience benefits from such preventive methods and treatment.
c. If you don’t have fixation and “pointing” in the extreme points of one part of your visual field it means that your agonist and antagonistic ocular muscles suffer from lack of strength and flexibility. Such a condition affects “central fixation/centralization,” or better focusing on the retinal part called the “fovea centralis,” which results in blurred vision. Impatience is a bad ally when the journey is very long and requires perseverance and patience.
d. Blinking and relaxation are two synonyms: since you have asked me this question it means that you didn’t understand the purpose of blinking—that is, ocular relaxation itself.
e. Keep on binocular fixation as long as you can: your nose is a physiological obstacle that must be “taken into account and respected”: it doesn’t mean that the exercise is less efficacious.
f. The therapists will come with time: ophthalmologists and opticians will become aware of this treatment’s importance, little
by little. I’m at their complete disposal, whenever they need me. The patient himself must be the one to ask for nonpalliative treatment. The patient will ask for “unconventional” methods, as such methods are considered today, and they will substitute for or, at least, add to the present conventional “treatments.” I hope I’ve satisfied your curiosity. My advice is always the same:
Practice, practice, practice!
For further information, please visit the Power Vision System website at www.powervisionsystem.com
or order the Book “The Secret of Perfect Vision”