
Originally published in Manhattan Eye and Ear Hospital Reports, vol. 2 (Jan. 1895), pp. 41-56
My attention was first called to this very interesting physiological question by a remarkable case of this kind which occurred in my private practice. On looking over the literature of the subject, I find the question of "accommodation in the lensless eye" still an unsettled one. Leading authorities - Helmholtz, Donders, Mannhardt - on the one hand, asserting that the lensless eye is devoid of accommodation, Donders* declaring that his "investigations had led him to the conviction, that in aphakia not the slightest degree of accommodative power remains." On the other hand, eminent authorities - Förster, Woinow, von Graefe, Loring - contend that accommodation does exist in aphakial eyes, Loring** affirming "that occasionally a considerable, if not a large degree of accommodation may exist, even in a lensless eye."
*Donders, Accom. and Refrac. of the Eye, 1864, p. 320.
**Flint, Physiology of Man, 1875, vol. v., pp. 110, 111.
Not only have these eminent authorities disagreed on the abstract point "of accommodation, or no accommodation in the lensless eye," but, unfortunately, those who have agreed on one side or the other, do not agree as to how, if present, it is brought about; or how, if not present, it still appears to be present. Undoubtedly the absence of the same or uniform tests accounts for a great deal of this difference of opinion. That some lensless eyes possess the power of adjusting themselves to seeing objects at different distances (call it accommodation, or what you will), with one and the same glass, and that glass held at one distance from the eye, there is no question in my mind whatever. How this adjustment or accommodation is brought about is quite a different question.
Besides my own case, I am able, through the courtesy of Dr. Webster, to report a similar case which occurred in his private practice.
CASE 1. Mr. E. C., aged 42, chef. On January 27, 1894, I removed a sclerosed or "black" cataract from his right eye, doing an iridectomy upward at the same time. His vision at time of operation was: R. E. 20/70, L. E. 20/40. Jaeger No. 12 at ten inches R. E., and Jaeger No. 9 at ten inches L. E. Though his vision was this good he could not recognize members of his family or friends on the street, had not worked for five years, and insisted on the operation being done. February 21st, about three and one half weeks after the operation, the ophthalmometer showed astigmatism with the rule 4.50 D, axis 90 + 180 -. April 20th, less than three months after the operation, the ophthalmometer showed absolutely no astigmatism. V. R. E. 20/10 (Snellen) With + 11.50 Ds. He read Jaeger No. 1 at ten inches with + 15.50 Ds. These glasses were accordingly ordered, + 11.50 Ds for distance, and + 15.50 D. for reading. I saw nothing more of the patient till six months later, October, 1894. The reason for his visit to me at this time was, not because the eyes were not doing well but because he thought he might be "straining" them; as he informed me he had been using his distance glasses all the lime, both for distance and reading, having discarded his reading glasses after a few weeks' use. I doubted the truth of his statement at first, never having seen such a case before. On testing his vision I found he could, with + 11.50 D., his distance glass, which I took the precaution to measure and verify, read 20/10 (Snellen); and with the same glass, held at the same distance on nose, he read Jaeger No. 1 from fourteen to eighteen inches. October 8, 1894, I presented the case in person before the New York Ophthalmological Society (before which he kindly consented to go). The members of the society were divided in their opinions as to how the patient was able to accommodate for the near point with his distance glasses on. February 4, 1895, I saw the patient again. He still read Snellen 20/10 -, and with same glass Jaeger No. 1 from eight to twenty-two and one half inches. This was such a remarkable increase in his relative range of accommodation for the near point, that I decided to make a thorough examination of his eye in every respect, accurate measurements of his cornea, and to ascertain, if possible, how such a result could be brought about. I accordingly subjected him to the following tests :
Subjective tests:.- 1 (a) Acuteness of vision for distance and near, point, with the distance glasses; (b) same with tipper lid held up ; (c) same with a few drops of cocaine instilled and speculum to hold lids open; (d) adding weak plus or minus glasses to his distant glasses and noting changes in acuteness of vision; (e) to repeat the above tests with the opposing eye uncovered, and with the visual lines converging. 2. Tested his acuteness of vision for a distant point of light (after Donders' method), tinder the five conditions imposed it) test No. 1.
Objective tests. - 1 (a) Measurement, with the ophthalmometer, of the radius of curvature of the two chief meridians of the cornea at the point where the visual line intersects same; (b) the same measurement five degrees to the outer side of this point, which was close to the apex of the cornea in each of the cases here reported, as the angle alpha was positive and about five degrees in each. 2 (a) With the Placido disc* removed from the cylinder of the ophthalmometer, and with the patient looking five degrees to the inner or nasal side, to note if any changes were made in the relative position and size of the corneal images when the eye changed from looking in the distance to a near point,** the eye not changing its direction; (b) the same test with lids held open with a speculum ; (c) with the opposite eye uncovered both of the above tests were repeated. 3. Ophthalmoscopic measurements of the fundus Were made to see if any change in depth occurred when the eye changed from a state of rest to accommodative efforts. 4. The size and shape of the pupil, if clear, or partially filled with membrane, activity, etc., were noted.
* Meyrowitz replaced this with a smaller disc placed back of the arc with the correct numbering and an indicator, so that the axis could be ascertained.
** The distant object at which the patient looked at in this test was the window of a house reflected from a French-plate mirror, which I had fixed on a revolving stand just back of me and facing the patient and window at which the ophthalmometer was placed. The houses reflected by the mirror were about one hundred feet distant, the eye observed being perfectly relaxed, therefore, when looking at them. The near point was a fine, black dot, 2 mm. in diameter, near the end of a narrow strip of white paper, which I pasted on the end of the tube, turning the strip of paper at a right angle to the tube and letting the end extend far enough to be five degrees from the centre of the tube. I pasted two of these slips on the tube, one to the side, one above. The distance from the end of tube to the observed eye was eight inches.
All of the above tests were repeated with the eye under the influence of a mydriatic.
The results of these tests in my case were: 1. V. R. E. = 20/10 (Snellen), with + 11.50 Ds (1 / 3-1/2). With the same glass, and without moving it on his nose, he read Jaeger No. 1 from eight to twenty-two and one-half inches, holding the type in the usual reading position, that is, slightly below the centre of the glass. he did not tilt his head or the glasses. When the type was held up higher, directly in front of glass, he could not read quite so well as when he held the print a little lower, as the print is held when reading naturally. I repeated this test time and again, and had Dr. M. L. Foster present on two occasions. Holding the lid up with the finger or with speculum made no change in his acuteness of vision whatever, either for distance or near. With the eye scopolamized (1/10 per cent. solution instilled every five minutes for thirty-five minutes, then a wait of one half hour), the distant vision was still 20/10 -, while the relative range for the near point, Jaeger No. 1, was nine to twenty-one inches; his relative range of accommodation for the near point was reduced but two and one half inches. When the left eye was covored in these tests, it was seen to turn in and the pupil to contract for the near point. Leaving the left eye uncovered made no change in any of the tests. A +.50 D. spherical glass added to his distant glass made him see worse for the distance ; with a -.50 D. spherical added he saw the same, while a -.75 D. spherical made him see worse. From this, it would seem that he had accommodative power to the extent .50 D., even forthe distance. 2. Having the patient look at a point of light (a portion of lamp flame seen through a round hole, 3 mm. in diameter, in a piece of cardboard) twenty feet distant with his distance glasses on and adding a + 1/263 ( (1/26 () - 1/32) made no change in the circle of light, neither did a + 1/160 (.25 D.). A +1/80(.50 D.) elongated the circle of light in the vertical meridian. It took a -1/80 to elongate the circle of light in the horizontal meridian. An effort of accommodation elongated the circle of light in the vertical meridian, just as the +1/80 spherical had done. When the lid was held up with finger, or with speculum, and when the eye was scopolamized, the test with the distant point of light was wholly unsatisfactory and contradictory. With the left eye uncovered and the right converging in the line of light, the tests were about the same as when the left eye was covered.
Objective tests. - 1. The ophthalmometer showed him to have absolutely no astigmatism. The radius of curvature at the point where the visual line intersected the cornea was 8.9 mm.; at the apex 9 mm. When the patient looked five degrees to the inner side of the tube (relative to the eye, the nasal side), just by the end of slip of paper I had pasted on the tube, into the distance; I approximated the images of the mires in the horizontal meridian so that they just touched. Then, without changing the direction of his eye, I had him focus on the black dot on the end of strip of paper. With his greatest effort at accommodation the images overlapped to the extent of one half diopter perhaps. The cornea moved forward a little, too, as was shown by the images getting out of focus, and the instrument had to be pulled slightly away from the eye in order to get them in perfect focus again. Or, if I had him focus on the black dot first and approximated the images, then let him look in the distance, the images separated slightly and the instrument had to be pushed toward the eye to get it in perfect focus again. Letting the patient look still in the same direction, but turning the arc of the instrument in the vertical meridian, and repeating the above experiments, the results were just reversed; that is, if I approximated the images while he was looking in the distance, then had him focus on the near point, the images separated slightly; but, if the images were approximated while he focused on the near point, and then looked in the distance, they overlapped about one half diopter. The same changes took place when the lids were held open with a speculum, and even when the ciliary muscle was paralyzed with scopolamine. The changes produced in his cornea must, therefore, have been produced by the action of the external muscles of the eye.
2. It was impossible to detect any change in the depth of the fundus of the eye with the ophthalmoscope when the eye changed from a state of rest from looking in the distance with opposite eye to a state of accommodation. The fundus of the eye was normal, with the media perfectly clear. 3. The shape of the pupil is an irregular oval, from the iridectorny, and free from membrane, except a very narrow margin at the edge, though, when I reported him to the New York Ophthalmological Society, and before I had made a critical examination, I had thought there was more membrane present. The transverse diameter of his pupil is 3-1/2 mm., the vertical about 7 mm. (see Fig. 1, A). B., Fig. 1, shows pupil dilated and some remains of membrane at periphery.
Case 2. Master W. 0. B.,* aged 13. School boy. Dr. Webster saw this patient first in Nov., 1891, when ten years of age, brought to him for double congenital cataract. The patient had already had eight discissions done on the left eye, the first one in Nov., 1890. When Dr. Webster saw him his vision was: R. V. = 20/70, no improvement with glasses. L. V. = 20/100, with + 10 D. November 28, 1891, Dr. Webster did a discission of the membrane in the left eye. January 19, 1892, L. V. = 20/70 with 13 D.
* This case, a private patient of Dr. Webster's, has been reported by him in a series of cases as: A Case of Congenital Cataract, both Lenses Removed by Operation, Arch. Pediatrics, New York, Nov., 1893, p. 432.
"As the patient saw with the right eye about as well without a glass as lie saw with the left with one, I concluded that he might as well go about without glasses for distant vision, and I gave him for reading, Right, plain glass. Left, +16 D.
"March 14, 1893. - The patient returned for further advice, and I found he was wearing the glasses all the time, which I had prescribed for reading only. On testing him I was surprised to find that with his left eye, with his glass, +16 D. he had Vision 20/20, while with the same glass he read Jaeger No. 1, at fourteen inches easily. This looked as though his aphakial eye still retained its power of accommodation."
Subsequently the right lens was removed by discission and linear incision, but no accommodation was observed, though his vision with a +13 D. was 20/50. I saw this patient first, March 16, 1895, and subjected him to the same tests as in my own case, with the following results: 1. V. R. E. - 20/300, with + 13 D. V. L. E. 20/20 -, with +16 D. Jaeger No . 8 , at ten inches, right; Jaeger No. 1, from ten to eighteen inches, left, with his distance glass, not moving it, and looking directly through its centre. His accommodation for the near point for the left eye had increased to ten inches from fourteen inches, since Dr. Webster saw him two years previously. His right eye, however, not only had no accommodative power for near point, but distantvision inithad decreased from 20/50 to 20/200, due to a membrane filling pupil. Holding the lid up with the finger, or with speculum, or even paralyzing the left eye with scopolamine did not change his vision for the distance or near point, he still seeing 20/20 - in distance, and Jaeger No. 1. ten to eighteen inches for the near point, but not quite so easily as before. With the right eye uncovered he could read more easily, but no better. Both + and - .50 D. spherical glasses added to his distant glass, made him see worse in the distance, especially the - .50 D. 2. Looking at a distant point of light and adding a +1/263 or -1/263 to his distance glass had no effect, neither was he positive of a change in the circle of light with a + or a - 1/160 (.25 D.). A + 1/80 (.50 D.) elongated the circle of light into a vertical oval. A a - 1/80 (.50 D.) elongated the circle of light into a horizontal oval. An effort at accommodation elongated the circle of light slightly in the vertical meridian. Holding the tipper lid up had but little effect in this test, but when the eye was under the mydriatic action of scopolamine, the tests for point of light were unsatisfactory.
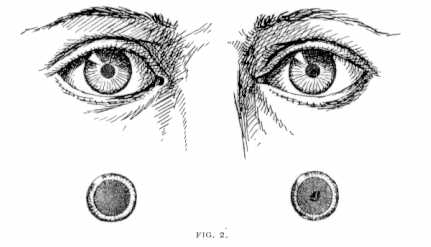
Objective tests. - 1. The ophthalmometer showed left eye to have astigmatism with the rule, 3 D. axis 65 + 155 -. The radius of curvature of the meridian at 155 was 8.5 mm., at 65 it was 7.9 mm. At the apex of the cornea the radius of curvature of the meridian at 155 was 8.5 mm., at 65 it was 7.85 mm. When this patient looked in the distance then focussed for the black dot on the end of paper, under the same conditions as in Case No. 1, there was absolutely no change in the relative positions or size of the corneal images. Furthermore, the images of the mires remained in perfect focus, showing that the cornea had not moved forward or backward. Leaving the right eye covered or uncovered made no difference in the tests. 2. The opthalmoscopic examination was the same as in Case No. 1 - negative, except to show that the fundus of the eye was normal and media clear. 3. Pupil circular (perhaps slightly oblong in the vertical meridian), active, 3-1/2 mm. in diameter, but considerably incroacbed upon at the inner side by a crescentic band of membrane, giving it somewhat the character of a stenopæeic slit. This slit was 2 mm. wide and 3-1/2 mm. long, and was crossed by two very fine threads of membrane, horizontally (see Fig. 2, A). When the pupil was widely dilated it was filled up entirely by a dense membrane, except the small central opening already described (see Fia. 2. A'.)
Such is the report of the two cases. The question, "How was the accommodation brought about in these cases?" presents itself for consideration. Before giving my own views, I wish, first, briefly, to present the views of some former writers on the subject. Ramsden and Horne* were arnong the first to examine aphakic eyes for accommodation. They were of the opinion that the accommodative power present in such cases was due to the cornea becoming more curved and moving forward at the same time. Thomas Young ** did not believe there was any accommodation left in the lensless eve, but was only tolerably well satisfied with his tests in proving its absence. Von Graefe *** was of the opinion that the aphakic eye retained some accommodative power. Helmholtz and Donders were quite positive that the lensless eye retained no accommodative power, and Donders **** declared himself very forcibly in his text-book on this subject, claiming that not trace of accommodative power remained in such cases. And later, in Graefe's Arch. of Ophthal., xix., p. 63, he still holds to this view. I do not consider Donders' tests, however, as conclusive, as the two which he based his conclusions on mainly were both subjeclive. To wit: 1. That an aphakic eye when accurately fitted for a distant point of light will see it as a circle, and where the patient makes the greatest accommodative efforts the shape of the light is not changed, but is only made smaller concentrically, due to a contraction of the iris; on the other hand, whien a weak plus or ininus glass (1/300) is placed before the eye, with its proper correction on, the circle of light is converted into a vertical or a horizontal oval. 2. That the acuteness of vision, with the distant-glass on, should be the same in a certain or stated interval, e.g., 1/2 for distance and 1/2 for some near point. By these two requirements of Donders, then, both of my cases had accommodative power left; for, as regards the first requirement, both, by accommodative effort, could convert the distant circle of light into a vertical oval. Furthermore, in each case it took as strong a glass as +1/80 to produce a like effect, and -1/80 to convert the circle into a horizontal oval (see test No. 2 above in each case). As to his second requirement: Case I. read with the same glass, + 11.50 D., Snellen X. at twenty feet, V. at ten feet, and Jaeger No. 1 at eight inches. Case II. read with the same glass, + 16. D., Snellen XX. at twenty feet, X. at ten feet, and Jaeger No. 1 at ten inches. Another case, reported by Dr. Silex, which will be referred to again, complied with both of Donders' requirements, so that it may be taken as proven that Donders' tests were wholly inadequate to decide the question at issue.
* Cited in Graefe-Samisch Augenheilk., Path.Therap., vol. v., p. 443
** Cited in Graefe-Samisch Augenheilk., Path.Therap., vol. v., p. 444
*** Loc. cit., p. 444. Also original article, Graefe's Arch. f. Ophthal., Bd. II., Abth. i., p. 188. **** Donders' Accom. and Refrac. of the Eye, p. 320.
In 1872 Professor Förster,* of Breslau, reported a series of twenty-two cases of apparent accommodation in aphakial eyes. They ranged in age from 11 to 74 years, the younger patients having more accommodative power than the older ones. His experiments were not decisive, however, as he did not leave the distance glasses on when he tested for the near point. Förster was of the opinion that the accommodative power present in these cases was due to the cornea becoming more curved. This was more or less of an assumption on his part, as he did not make the proper objective tests to prove his statement. However, that the curve of the cornea can be changed, by accommodative effort, to a slight extent at least, in the lensless eye, is shown by my case. In the normal eye the change in curvature of the cornea, by accommodative effort, is some cases very marked. The most rnarked case of this kind that I have seen occurred in the person of Dr. C. H. Johnson, a former House-surgeon at the Manhattan Eye and Ear Hospital. The ophthalmometer showed him to have ordinarily an astigmatism .50 D. ax. 90+ 180-, both eyes. He could, however, without in any way changing the direction of his eye, voluntarily, by efforts at accommodation, change this in the right eye to 2 D., and in the left to 1.50 D. he was able to do this while the upper lid was held up with the finger, showing that it was not due to lid-pressure. He did this many times, and the same change was observed by a number of the staff at the hospital. Desiring to know if this change was due to the action of the ciliary muscle or to that of the external muscles of the eye, I wrote to Dr. J. M. Ray of Louisville, where Dr. Johnson now resides, to put Dr. Johnson's eyes under the influence of a mydriatic (the doctor permitting), and in that way eliminate the question of the ciliary muscle. I give his report:
*Klin. Monatsbl. f. Augenheilk., Erlangen, 1872, B.X., p. 39 et seq.
V.R.E. = 20/20; V.L.E. = 20/20. Ophthalmometer shows astigmatism with the rule .50 1). ax. 70 + 160 - Rt. ; 90 + 180 - Lt. "When he made an effort at accommodation without changing the direction of his eye, the astigmatism can be seen to go up to 2 D. in Rt., and 1.50 D. in Lt. Scopolamine, four instillations of 1/2 per cent. solution, apparently paralyzed accommodation. Then with the ophthalmometer the astigmatism still seems to increase in the right eye to 1.50 D., and in the left to 1. D."
From this it appears that, in Dr. Johnson's case at least, the change in the curve of the cornea is brought about mainly by the external muscles of the eye, as the influence of the lids and ciliary muscle was eliminated. Again, in my case, the external muscles must have caused the slight change which took place in the cornea, as when his eye was under the influence of a mydriatic the change could still be observed.
Woinow* reported a series of eleven cases of accominodation in the lensless eye in 1873. The patients ranged in age from 12 to 60 years. The fault in the tests of Woinow's cases consisted in the fact that he took the relative range of accommodation for the near point only. This relative range was comparatively small, amounting in no case to more than six inches (see loc. cit., p. 116), and averaged on the whole about 1/20. He failed also to make adequate objective tests, and in closing his paper acknowledges he can give no positive answer as to the cause of accommodation in aphakial eyes, but believes it was due to three factors: 1. To the anterior surface of the vitreous becoming convex after the lens is removed, and in that way acting as a plus lens, 2. To the action of the ciliary muscle and a change in the depth of fundus from that action. 3. Action on the globe of the eye of the external muscles. He thought, also, that a change in the curvature of cornea [night be a factor, but finally eliminated that.
*Arch. f. Ophthal., Berlin, 1873, Bd. xix, p. 107 et seq.
As to his first factor, that the anterior surface of the vitreous became more convex after the lens was removed (which he discovered in two cases by a weak image reflected from it in the upright position), and in that way acted as a plus lens to converge rays of light, I think he is mistaken. This simply from the fact that the index of refraction of the cornea, aqueous and vitreous, is the same for each, and, consequently, as pointed out by Donders,* "we have in the aphakial eye only one refracting surface to take into account, namely, the anterior surface of the cornea," As to his second factor, I believe the ciliary muscle has but little effect on the depth of the eye. I am brought to this conclusion because, when the ciliary muscle was paralyzed in the two cases that are reported by me, the accommodation remained exactly the same in one as before the mydriate was used, and was reduced but about two inches in the other. Furthermore, he states in his own paper that a quota of accommodation remains in such eyes after they have been atropinized, e.g., where it was 1/28 before using atropine, after using it the accommodation was 1/40. As to the third factor, I believe the action of the external muscles do have some slight effect in changing the length of the eye in aphakia, but very little, if we can judge from my first case. In the normal eye they may have more effect, as shown in Dr. Johnson's case.
*Donders, Accom. and Refrac. of the Eye,, p. 310.
Loring reported a remarkable case of accommodation in the lensless eye to the New York Ophthalmological Society, April, 1879, and the same case to the American Ophthalmological Society in 1870. He later reported the same case at length for Flint's Physiology of Man, p: 110 et seq. Roosa quotes the case in full in his text-book, A Clinical Manual of Diseases of the Eye, p. 57.
Loring's case occurred in the person of a young woman, 18 years of age, who had had both lenses removed by discission five years previous to his seeing her. "The pupils were round, free from membrane and active. With + 1 / 3 1/2, the patient read with either eye fluently Snellen XXX. and was able, with both eyes, to pick out most of the letters of XX. at twenty feet. She could read No. X. at ten feet, and No. V. at five feet. With the same glass, and with no change of position on the nose, she read No. 1 1/2 Snellen fluently, holding the book naturally at twelve inches, which was about the distance at which she usually read. The book was then gradually withdrawn, the patient reading aloud while this was done. It was found that twenty-one and a half inches was the greatest distance at which No. 1 1/2 Snellen could be read. She read No. 1 Jaeger at twenty inches. The book was then advanced inch by inch, the patient reading aloud, till the book was within five inches of the eye. Inside of this reading was impossible. These experinieuts were tried over and over again by myself, and were finally repeated in the presence of a brother oculist. This would give the patient an adaptability of the eye for different distances from twenty feet (or parallel rays) to five inches; or, in other words, an accommodation of 1/5 (A=1/5), and a relative accommodation for the very finest print from twenty inches to five (A= 1 / 6-1/2)."
Loring also cites the papers of Förster, and Woinow, already quoted in this paper; also a paper by Arlt* in which is reported the case of a younge man who had after cataract extraction a marked amount of accommodation left. "With convex 1 / 3-1/2, could read both at six and at twenty-four inches, and could recognize the hands of a steeple-clock, at a distance of more than five hundred paces, with the same glasses: but, as neither the size of the print nor that of the clock is given, no accurate calculations can be drawn from the case." Commenting on his own case Loring says: "The case observed by me would then appear to be the first - as it is certainly the most remarkable - subjected to the recognized standard test of vision."Die Krankheiten des Auges, Prag., 1858, bd. ii., S. 348.
Unfortunately even with the report of so remarkable a case, Loring, like al lbefore him, failed to make adequate objective tests, and so left the question of accommodation in the lensless eye unsettled. His patient promised to return to have these further tests made, but failed to do so. Loring's remark (through no fault of his own, however,) on Woinow's and Förster's failure to amke the proper objective tests applies with equal force to himself, e.g., "It is to be regretted, and it certainly appears a little strange, that in neither Förster's nor Woinow's cases, was either the optometer or ophthalmoscope used in the elucidation of this problem." Withal, however, he was of the opinion, "that occasionally a considerable, if not a large degree of accommodation may exist, even in the lensless eye."
Dr. Paul Silex's* paper "On the Question of Accommodation in the Aphakial Eye," in 1889, is thelatest rontribution on this subject with which I am acquainted. Some cases observed in the Berlin eye clinic induced him to make a careful examination into the subject.
The most marked case occurred in a boy, aged 14, who had had a cataract removed five years previously by repeated disscissions. This patient complied with both of Donder's requirements, that is, his acuteness of vision was the same in a given interval, e.g., distant vision was 6/12 = 1/2, and his near vision was 25/50=1/2. And as to the slight point test Silex observes that it was just the reverse in this case. When he had classes of slight value added to his distance glass the patient gave contradictory answers, but efforts at accommodation on the intersection of two fine threads near at hand, and in the line of vision of the observed eye for the distant point of light, changed the light into a vertical oval. Silex did not depend on these two requirements, but made objective tests with the ophthalmometer. I mus confess, hovewer, that I do not understand his method of testing with that instrument. He says: "The patient left his glasses on, as without them his fixation would have been unsteady. He had to look alternately at the tube of the instrument and at small printed pieces of paper held at reading distance from his eye a little down and in. In spite of the eighteen reflected images of the lamps, it was easy to distinguish those belonging to the cornea. The pupil contracted on convergence, the boy alleged to recognize the letters clearly, but the relative position of the images did not charge."*Knapp's Arch. Ophthal., vol xviii., p. 274: translated by H. Knapp.
First, I do not understand how the cornea ws measured when the patient "kept his spectacles on." I have never seen it done, but perhaps I am unfortunate in that respect. It seems to me, too, that eighteen reflected images would be a little confusing, and make it anything but easy to distinguish those belonging to the cornea. Second, he says, "the relative position of the images did not change," and this, though the patient first looked at the tube then a little down and in at printed pieces of paper. This is wholly contrary to my experience with the use of the instrument. My experience has been that the least change in the direction of the eye changes the relative position of the corneal images. In fact, one of the chief precautions laid down as a guide in the use of the instrument, is that the observedeye shall look steadily at the centre of the tube; the leaste change from this, as a rule, causes a change in the relative position of the corneal images. By a change of direction of the eye of five degrees from the centre of the tube, I have a change of as much as one diopter in the amount of astigmatism; and for ten degrees, as much as two diopters. How far the doctor means by "a little down and in," I do not know, but, if as much as ten degrees, he certainly measured different points on the cornea, and his test would not hold. His conclusions from the tests were, "that the aphakial eye was devoid of accommodation," and the ability to read at near point in thise cases was due in the main, "to the unusual faculty of certain ametropes to overcome dispersion circles."
My own conclusion, from studying the history of the subject, and from the careful and complete tests made in the two cases here reported, is, That the accommodation present in the lensless eye is due chiefly if not solely to the ability of the patient in such cases, to interpret dispersion circles. The slight change in curvature of the cornea, and its slight advancement observed in some cases, may, in those cases account for some of the accommodative power present, but it is such a small factor that it may be eliminated entirely, especially since in some of the most marked cases of accommodation in aphakial eyes no such changes have been observed. How the change in the curvature of the cornea and its advancement are brought abount, have been discussed in this paper already.
Although, as Loring says, "It would seem impossible that the ability to read the finest print at five inches (which was done in his case), even taking into consideration the magnifying power of the class, could be due to the overcoming of the circles of dispersion," yet I believe such to be the case, and for the following reasons: First, to the great increase in size of the retinal images by the removal of the crystalline lens and replacing it with a lens in front of the eye. By this procedur the united nodal point is removed forward, and this, with the magnifying power of the glass in front of the eye, greatly increases in size the retinal images. Donders* has shown by calculation, that a convex lens of three inch focus, placed one half inch (usual distance) in front of the eye increases the retinal images in size one and one third times. By this one factor alone, then, the images of Jaeger No. 1. would be increased in size until they equalled (for the unoperated eye) Jaeger No. 2 or a little larger. Second, to the narrowing of the pupil. Where no iridectomy is done, this is due to the contraction of the iris as the result of convergence and an effort at accommodation; where an iridectomy is done to a partial filling up of the pupil by membrane, except a central opening. It is a well known fact that if the pupil is narrowed from any cause such narrowing acts as a diaphragm to cut off the peripheral rays fo light entering the eye, and serves in this way to lessen the dispersion circles. Third, to the extraordinary acuteness of vision present sometimes present after cataract extractions, e.g., as happened in my case, where it was 20/10, double the ordinary acuteness of vision. I believe this fact contributed largely to the power of interpretation present in this case; for he had an iridectomy and a clear pupil. Fourth, in some cases, to the patient not looking directly through the centre of the glass, but slightly outside of the centre, either by tilting the glasses, tilting his head, or not holding the reading matter directly in front of him. In my opinion, this fourth factor - in effect, a slight tilting of the strong pluss glasses - assists the individual in interpreting dispersion circles chiefly by neutralizing the monochromatic aberration present in such cases. This is a point which no writer has hitherto called attention to in discussing this subject. Wm. Harkness* has shown that, "with a pupil four millimetres in diameter, the normal cornea produces monochromatic abberation to the extent of 1/33: and as there is no confusion of images in the normal eye, it seems probable that the crystalline lens exerts some compensating action. This suspicion is strengthened by the well-known fact that in aphakia, the acuteness of vision is nearly always improved by giving a certain inclination to the powerful convex glasses which are then necessary." Furthermore, this very fact of monochromatic abberration in the lensless eye, to my mind renders Donders' Light-point test more or less unreliable.
In conclusion, I might say that I believe this question of accommodation in the lensless eye would have been settled long ago had the proper objective tests been made. From one cause or another, not a single observer made all the tests necessary to settle the question, except for himself, and some did not succeed even in doing that. In fact, all of them together failed to make the requisite number of tests. Dr. Silex came nearer to it than any who had gone before, but he failed in one most esential feature, and that was to atropinize his subjects. Besides his one objective test was open to serious objections in its technique. Most of the observers were content to rest the case on mere assumptions and subjective tests. Even that most careful of observers, Denders, fell into this error; so that, the quotation he once applied to Wharton Jones and Wilde, in regard to their assertion, "that the radius of curvature of the cornea was shorter in the vertical meridian than in the horizontal," before they had proved it (even questioning if they should receive credit for their observation), can be equally as well applied to himself, and others along with him who had the same opinion in regard to accommodation in the lensless eye. The quotation was, "We see that in science also the quotation is sometimes appliccable, that 'audaces fortuna juvat.'"
They were right, I believe in their assumption, but failing to bring sufficient evidence to prove it, still left the question of accommodation in the lensless eye and its cause sub judice.
* Knapp's Arch. Ophthal., vol. xii., p. 18.
** Donders, Accommodation and Refraction of the Eye, p. 543.